
Overview
Mental health is a key part of wellbeing. The government plays an important role in managing the funding of mental health, alcohol, and other drug services, initiatives, and infrastructure. This supports people to maintain wellbeing, receive treatment, and to recover from mental illness and the problematic use of alcohol and other drugs.
This audit focused on how:
- the levy is managed as a whole across the mental health, alcohol and other drugs system
- Queensland Treasury and the Department of Health manage their respective responsibilities for the levy.
Tabled 22 May 2026.


Report summary
This report examines whether Queensland’s mental health levy is effectively managed to achieve its intended purposes. This audit focused on:
- the management of the levy as a whole across the mental health, alcohol and other drugs (MHAOD) system
- how Queensland Treasury and the Department of Health manage their respective responsibilities for the levy.

| What is important to know about this audit? |
Queensland’s mental health levy was introduced in 2023. Its intended purposes are to:
- increase funding and expenditure on MHAOD services
- respond to emerging needs by enhancing existing services and introducing new services
- reform Queensland’s MHAOD system.
The levy can only be spent on specific services or infrastructure under legislation. The Queensland Government allocates levy funding to government entities to deliver and manage MHAOD services in Queensland. These services support people to maintain wellbeing, receive treatment, and recover from mental illness and problematic use of alcohol and other drugs. These entities and services collectively make up the MHAOD system. Queensland Treasury is responsible for administering levy funding.
Since its introduction, the levy has raised substantial revenue for Queensland’s MHAOD system.
Compiled by the Queensland Audit Office using information from Queensland Treasury and the Department of Health.

| What did we find? |
There is no coordinated approach to managing the levy as a whole.
The Queensland Government has not established appropriate structures, decision-making authorities, responsibilities, systems, and processes to effectively govern the levy as a whole. As a result, there is no whole-of-levy management approach, including:
- shared understanding between Queensland Treasury, the Department of Health, and the Queensland Mental Health Commission about what services and infrastructure levy funding can be used for
- planning to inform decisions about how funding is and could best be allocated across the MHAOD system
- monitoring how all funding is spent and whether the levy’s intended purposes are being achieved
- reporting on the levy to inform parliament and the public about its use.
Queensland Treasury is responsible for informing government decisions on funding submissions and administering allocated funds to entities. But it does not track all levy expenditure and there are gaps in how it administers funding. Entities are responsible for monitoring performance and expenditure for their levy-funded services, however, there is no consolidated understanding of how all levy funding has been spent or whether it has been effective.
The gap in whole-of-levy planning means that funding may not be targeted to achieve the levy’s intended purposes.
There is no coordinated approach to planning how all levy funding should be targeted across the MHAOD system to inform government decision making. Instead, the government has made decisions to allocate levy funding in response to entity requests. Some entities have undertaken planning to inform their requests for funding. This includes the Department of Health, which is responsible for planning and managing levy funding for specialised MHAOD services.
However, there is no coordinated approach to informing the level of funding directed across preventative, primary, and specialised MHAOD services to meet the levy’s intended purposes.
Most levy funding has gone to specialised services which focus on treatment and support for people experiencing mental illness or problematic alcohol and other drug use. The levy has also funded initiatives that support mental health and wellbeing, and help people who are experiencing, or who are at risk of, MHAOD issues. Levy funding has been used to replace existing funding sources for some initiatives.
Accurate data about levy performance or expenditure across all programs is not available. This makes it difficult for the government to assess the impact of the levy’s investment and understand whether it is driving reform in the MHAOD system as intended.
As the largest recipient of levy funds, the Department of Health manages most of its funding well, but can improve its governance approach.
The Department of Health designed a governance approach for its largest allocation of funding under its 5-year statewide MHAOD services plan, Better Care Together: A plan for Queensland’s state-funded mental health, alcohol and other drug services to 2027 (Better Care Together). However, there were gaps in the design and implementation of this approach that reduced its effectiveness. The Department of Health also designed a process to manage funding release under Better Care Together, which generally works well.
The Department of Health has increased outputs for specialised MHAOD services, but does not yet know if its programs are contributing to intended outcomes.
The Department of Health’s levy allocation has contributed to increases in key outputs including expenditure, beds, and employee numbers in Queensland’s specialised MHAOD system. However, the Department of Health does not yet know if its programs are contributing to their intended outcomes. This is primarily due to delays in its evaluation and gaps in its approach to measuring performance across all programs. Improvements to some health and wellbeing outcomes may only be evident in the longer term.
The Department of Health has spent 89 per cent of its allocated funding for Better Care Together from 2022–23 to 2024–25. It deferred $93.6 million in operational funding and $120.5 million in capital funding in 2024–25.

| What do entities need to do? |
We recommend:
- Queensland Treasury consults with key entities to establish coordinated governance of the levy as a whole, including by assigning roles and responsibilities
- Queensland Treasury strengthens how it administers levy funding by improving processes and establishing guidelines for entities that receive funding
- the Department of Health improves how it governs its total allocation of levy funding and informs future levy investment using its planning processes.
1. Audit conclusions
The mental health levy is not effectively managed as a whole to achieve its intended purposes.
This is because effective governance arrangements for the levy were not established when it was introduced. This included not defining the scope of the levy’s use, its outcomes, and responsibilities for:
- planning funding across the mental health, alcohol and other drugs (MHAOD) system to maximise its impact
- monitoring and reporting of levy performance and expenditure.
As a result, there is no consolidated view of whether the levy as a whole is allocated appropriately to maximise its effectiveness in reforming and increasing services and infrastructure across the MHAOD system.
Queensland Treasury and the Department of Health have each designed processes and systems aligned with their respective responsibilities for managing the levy. However, there are opportunities for both entities to improve how they govern and oversee levy funding.
Establishing effective governance arrangements, particularly at a whole-of-levy level, will enable planning and evaluation of how the levy is allocated to MHAOD services. This will help the Queensland Government to optimise levy investment and performance across the MHAOD system.
2. Recommendations
We have directed the recommendations in the report to Queensland Treasury and the Department of Health.
| Managing the mental health levy | Entity responses |
We recommend that Queensland Treasury:
| Agree |
| Agree |
| Agree |
| Using the Department of Health’s levy allocation to deliver outcomes | Entity responses |
We recommend that the Department of Health:
| Agree |
| Agree |
Reference to comments
In accordance with s. 64 of the Auditor-General Act 2009, we provided a copy of this report to relevant entities. In reaching our conclusions, we considered their views and represented them to the extent we deemed relevant and warranted. Any formal responses from the entities are at Appendix A.
3. Queensland’s mental health levy
Mental health in Queensland
Mental health is a key part of overall wellbeing. Mental illness is an issue that affects many Australians. It can have significant social, emotional, financial, and other impacts on the affected individual, their family and friends, and the broader community.
In Queensland, mental health, alcohol and other drugs (MHAOD) funding goes to services, initiatives, and infrastructure that:
- provide treatment and support for people experiencing mental illness and problematic substance use, their families, and carers
- promote and aim to improve mental health and wellbeing.
The World Health Organization defines mental health as a state of mental wellbeing. Mental health enables people to cope with stress, learn and work productively, and contribute to their communities.
A mental illness can be defined as a clinically diagnosable disorder that severely interferes with a person’s cognitive, emotional, or social abilities.
Queensland Audit Office using information from the Mental Health Select Committee’s Report No. 1, 57th Parliament – Inquiry into the opportunities to improve mental health outcomes for Queenslanders.
The mental health, alcohol and other drugs system operates on a continuum of care
MHAOD services are delivered across a continuum of care. The continuum recognises that people’s mental health needs change over time, with services organised to match the level of support they need. Services at one end of the continuum promote mental health and wellbeing and aim to prevent people from becoming mentally ill. Services at the other end are designed to treat people with severe and complex mental health needs.
The Queensland Government works with the Australian Government, private businesses, and non‑government organisations (NGOs) to provide MHAOD services that address Queenslanders’ needs.
Figure 3B shows the MHAOD continuum of care and identifies entities that deliver services across this system.
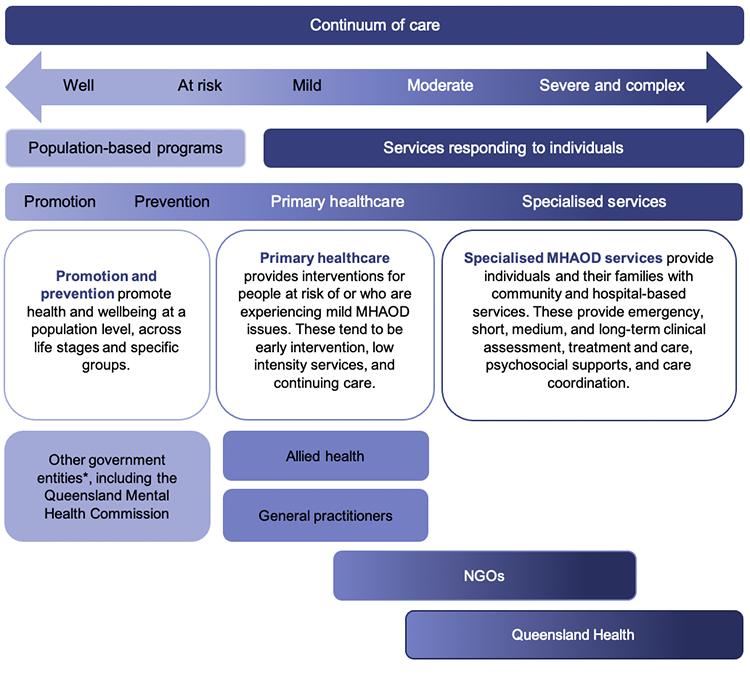
Note: * Other government entities include departments like the Department of Housing and Public Works and the Department of Youth Justice and Victim Support.
Compiled by the Queensland Audit Office based on information from the Department of Health and Queensland Treasury.
The mental health levy explained
The Queensland Parliament established the Mental Health Select Committee in December 2021 to conduct an inquiry into the opportunities to improve mental health outcomes for Queenslanders (the inquiry).
The inquiry resulted in 57 recommendations, including for the Queensland Government to create a dedicated funding stream for MHAOD services. The mental health levy was introduced in January 2023 to address this recommendation.
The levy is collected through payroll taxes. The Queensland Revenue Office, which is part of Queensland Treasury, budgets, collects, and reports on levy revenue. The levy does not have a prescribed end date, so it will continue to generate revenue indefinitely.
The levy’s intended purposes
The levy’s intended purposes are to:
- increase funding and expenditure for MHAOD services in Queensland
- enhance existing services
- introduce new services to meet emerging needs across the continuum of care
- reform Queensland’s MHAOD system through a substantial increase in investment.
The inquiry also emphasised the importance of government entities working in partnership to deliver services across the MHAOD system and improve outcomes for Queenslanders.
The levy has a prescribed use under legislation
The Payroll Tax Act 1971 states that levy funds must be spent on services or infrastructure that are consistent with either the:
- main objects and principles of the Mental Health Act 2016
- guiding principles in the Queensland Mental Health Commission Act 2013.
The main objects of the Mental Health Act 2016 primarily provide for people who have a mental illness and who do not have the capacity to consent to be treated, and people who were of unsound mind at the time of committing an unlawful act.
The Queensland Mental Health Commission Act 2013 includes broader principles regarding the rights of people who have a mental illness or misuse substances, and carers of these people.
One of the principles of this Act states that an effective mental health and substance misuse system is the shared responsibility of the government and non-government sectors. It states that this requires a coordinated and integrated approach, including across the areas of health, housing, employment, education, justice, and policing.
The levy is raising more funding than expected
The levy raised $1.2 billion from 1 January 2023 to 30 June 2025.
Figure 3C shows that Queensland Treasury projects the levy will raise $553 million more than originally estimated in its first 5 years. This is due to Queensland’s strong labour market and growth in wage inflation.
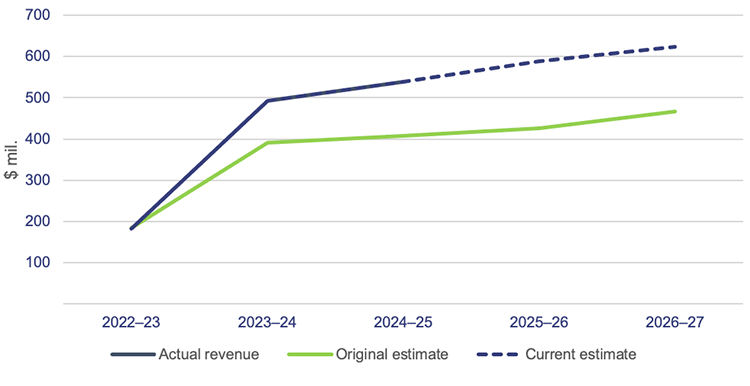
Note: The original estimates for 2022–23 to 2025–26 are from the 2022–23 Queensland Budget. The 2026–27 original estimate is from the 2023–24 Queensland Budget. As the levy came into effect in January 2023, the 2022–23 figure captures revenue for the period from January to June 2023.
Compiled by the Queensland Audit Office based on data from Queensland Treasury.
Funding has gone to several entities to manage and deliver MHAOD services
Approximately 92 per cent of levy revenue from 2022–23 to 2026–27 has been allocated to the Department of Health. The Department of Health transfers most of this funding to hospital and health services (HHSs), NGOs, and other government entities.
The majority of the Department of Health’s funding supports improving MHAOD services through Better Care Together: A plan for Queensland’s state-funded mental health, alcohol and other drug services to 2027 (Better Care Together). This includes funding to:
- respond to the inquiry, which includes mental health promotion and prevention initiatives delivered by the Queensland Mental Health Commission, the Department of Housing and Public Works, the Department of Trade, Employment and Training, Health and Wellbeing Queensland, and the Department of Youth Justice and Victim Support
- deliver initiatives beyond the health system under the Queensland Mental Health Commission’s Achieving balance: The Queensland Alcohol and Other Drugs Plan 2022–2027 and Every life: The Queensland Suicide Prevention Plan
- contribute to the Australian Government’s Bilateral Schedule on Mental Health and Suicide Prevention.
Funding is also used to:
- deliver initiatives in the Queensland Women and Girl’s Health Strategy 2032 (Women and Girls’ Strategy)
- support Queensland Government election commitments.
Some of the remaining funding is unallocated, and some has been provided directly to other government entities. This includes the Queensland Reconstruction Authority for disaster recovery programs, and the Department of Justice for a domestic and family violence related initiative.
Figure 3D summarises revenue and funding allocations from the levy for 2022–23 to 2026–27.
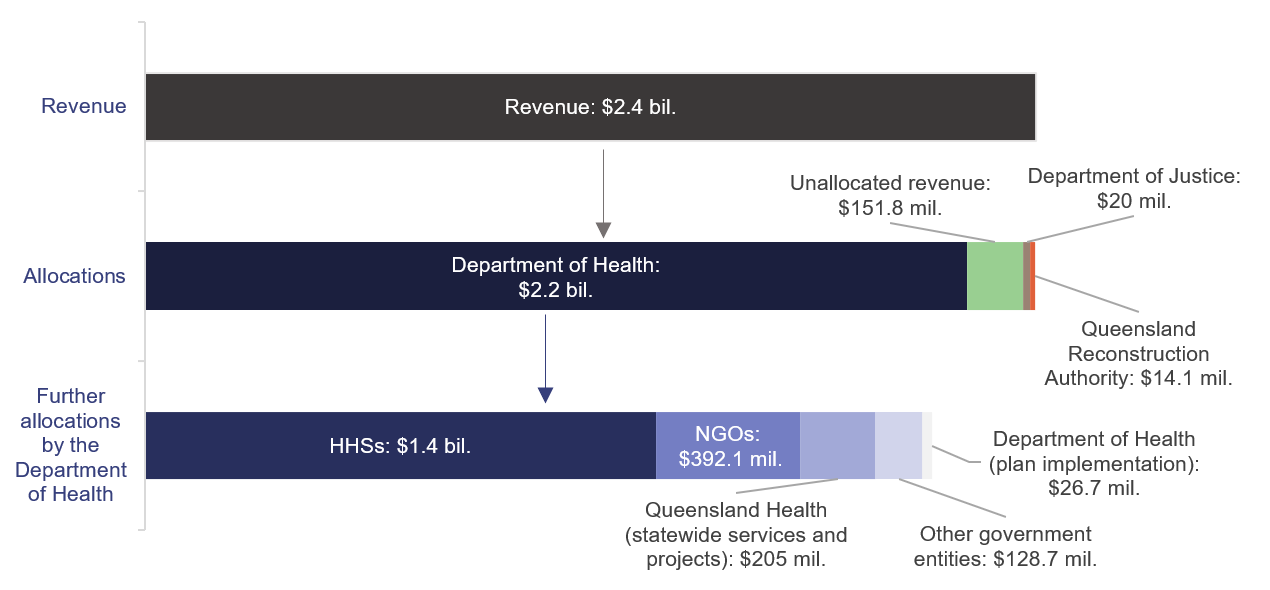
Note: The first bar summarises actual revenue for 2022–23 to 2024–25 and forecast revenue for 2025–26 and 2026–27.
The second bar summarises levy allocations as of February 2026, not actual expenditure. The Department of Justice allocation was transferred to the Department of Families, Seniors, Disability Services and Child Safety following machinery of government changes in November 2024. The second bar also includes funding allocations under Better Care Together and the Women and Girls’ Strategy.
The third bar summarises the Department of Health’s further allocations to different entities. Of the funding to ‘other government entities’, about $78.3 million has been allocated to the Queensland Mental Health Commission.
Compiled by the Queensland Audit Office based on data from Queensland Treasury and the Department of Health.
Managing the levy and services
Several entities are involved in managing funding and expenditure of the levy and delivery of MHAOD services in Queensland.
Queensland Treasury administers all levy funding
Queensland Treasury provides advice to the Cabinet Budget Review Committee on entity requests for levy funding through the state budget process. The Department of the Premier and Cabinet and other agencies also provide advice.
The Cabinet Budget Review Committee makes decisions to allocate funding from the levy. The Premier, Deputy Premier, and Treasurer are standing ministers of the committee. Other senior ministers are appointed as members as determined by the Premier.
Queensland Treasury is also responsible for the financial administration of levy funds, including:
- releasing allocated funds to entities in line with Cabinet Budget Review Committee decisions
- overseeing how much levy funding has been spent by entities.
The Department of Health manages the largest allocation of funding
The Department of Health is responsible for planning services delivered in the public health system in Queensland. These are typically specialised MHAOD services for people with moderate to severe mental health needs or substance use.
For the levy, the Department of Health is also responsible for:
- further allocating levy funding to other entities, including HHSs
- managing performance of its levy-funded initiatives
- reporting its expenditure and requesting deferrals from Queensland Treasury.
Hospital and health services
HHSs are part of Queensland Health. They deliver MHAOD treatment services in hospital and community-based settings. Fifteen of the 16 HHSs in Queensland deliver services within a specific region. Children’s Health Queensland delivers services for children and adolescents across Queensland.
Other entities manage and deliver services with levy funding
Queensland Mental Health Commission
The Queensland Mental Health Commission develops and monitors a whole-of-government strategic plan for improving MHAOD outcomes. The current plan is called Shifting Minds: The Queensland Mental Health, Alcohol and Other Drugs, and Suicide Prevention Strategic Plan 2023–2028.
The Queensland Mental Health Commission has received levy funding to deliver initiatives focused on social determinants and promoting health and wellbeing. These form part of the Queensland Government’s response to recommendations from the inquiry.
The Queensland Mental Health Commission does not currently have a role in governing the levy or planning how levy funds are invested across the MHAOD system. However, it participated in the Department of Health’s governance arrangements for Better Care Together as a member of its assurance and reference committees.
Non-government organisations
NGOs provide mental health services in a community setting. This can include counselling, peer groups, and other wraparound support. NGOs also provide alcohol and other drug treatment services including residential rehabilitation, withdrawal management, and psychosocial support.
Other government entities
The Queensland Government funds and delivers a range of mental health supports and programs through housing, education, employment, disability, and other social, justice, and community entities. This includes the Queensland Reconstruction Authority and the Department of Justice.
What did we audit?
In this audit, we assessed whether the mental health levy is effectively managed to achieve its intended purposes.
We audited:
- Queensland Treasury, focusing on the health and care team responsible for managing levy funding
- the Department of Health as the entity that has received the most levy funding to date.
We engaged with the Queensland Mental Health Commission and all HHSs. We also consulted with stakeholders in the government and community sectors.
Appendix B provides more detail on our audit scope and methodology.
4. Managing the mental health levy
Many entities deliver mental health, alcohol and other drugs (MHAOD) services across the continuum of care. Collectively, these entities and services make up the MHAOD system.
The levy is a significant financial investment. Given the range of services and entities involved, the levy requires clear responsibilities and coordinated planning to achieve its intended purposes.
In this chapter, we report on the governance and management of the levy as a whole and how funding is allocated across all aspects of the mental health continuum. We also examine how information about the levy’s effectiveness is monitored and used to inform future allocation decisions.
Is the levy effectively managed?
The mental health levy is not being effectively managed at a whole-of-levy level. This is because the government did not establish effective governance arrangements when the levy was introduced. There is no coordinated approach for planning and monitoring how funding is invested to achieve intended outcomes.
As a result, there is no:
- coordinated planning to identify how levy funding should be used across the continuum of care to inform government decision-making. Instead, funding is allocated in response to entity-level planning and requests, and is subject to different interpretations about how levy funding can be used.
- oversight or reporting about how all levy funding is spent and whether it is achieving its intended purposes.
There is no coordinated approach to managing the levy as a whole
Queensland Treasury and the Department of Health understand their respective responsibilities in managing the mental health levy. However, there are gaps in key roles and responsibilities for the levy as a whole, including planning and oversight.
Despite its role in the MHAOD system, the Queensland Mental Health Commission does not play a role in governing the levy as a whole. The Queensland Mental Health Commission participated in the Department of Health’s governance structure for Better Care Together: A plan for Queensland’s state-funded mental health, alcohol and other drug services to 2027 (Better Care Together). Its Achieving balance: The Queensland Alcohol and Other Drugs Plan 2022–2027 and Every life: The Queensland Suicide Prevention Plan, were considered when developing Better Care Together. However, the Queensland Mental Health Commission has not had a role in informing how the levy as a whole is allocated.
Figure 4A shows key levy responsibilities and current gaps.
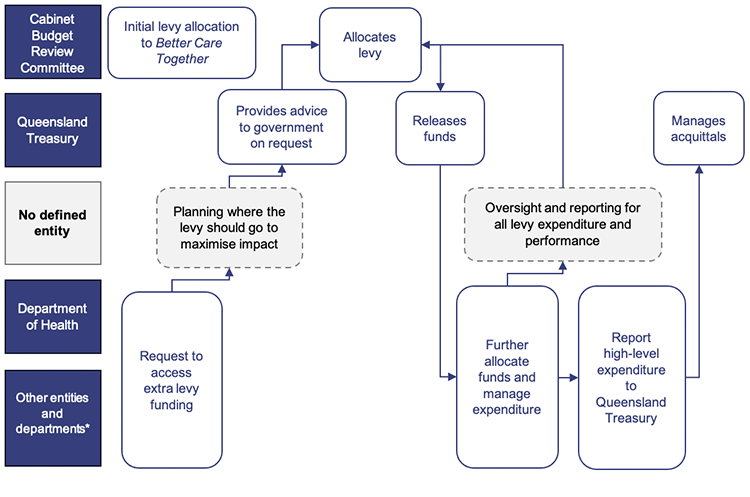
Note: * Other entities and departments include the Queensland Reconstruction Authority and the Department of Justice. The Department of Justice allocation was transferred to the Department of Families, Seniors, Disability Services and Child Safety following machinery of government changes in November 2024.
Compiled by the Queensland Audit Office based on information from audited entities.
There is no whole-of-levy approach to planning investment
There is no shared understanding about the scope of the levy’s use
There is no agreement between responsible agencies about how the levy can, or should, be used under the Payroll Tax Act 1971 (the Act). This is because an agreed interpretation of the scope of the levy’s use was not established at the time it was introduced.
The Act references broad principles, and responsible entities have interpreted these differently. The Department of Health holds a view that the legislation focuses on people who have a mental illness or who misuse substances, and their carers. Queensland Treasury and the Queensland Mental Health Commission consider broader activities that support mental wellbeing to also be within the scope of the levy. For example, Queensland Treasury’s advice endorsed funding to be allocated to disaster recovery and Queensland Women and Girl’s Health Strategy 2032 (Women and Girls’ Strategy) initiatives, which span across the continuum of care.
Without clarity on the scope of the levy’s use, it is difficult to plan and know whether funding is being directed to the right areas across the continuum of care. Instead, funding is allocated in response to funding requests and advice, which are based on entities’ individual interpretations of the legislation. Figure 4B shows that most levy funding has been allocated to specialised MHAOD services to date.
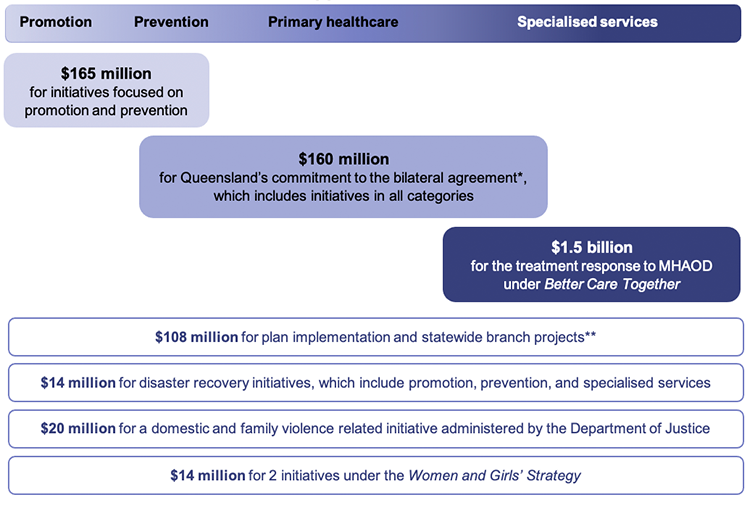
Note: Figures summarise decisions to allocate levy funding to operational initiatives from 2022–23 to 2026–27. The figures do not show actual expenditure. These figures exclude capital allocations. We could not map the 4 boxes at the bottom of the graphic to a single category on the continuum. Similarly, parts of some services may span across categories.
* The bilateral agreement refers to the Bilateral Schedule on Mental Health and Suicide Prevention between the Commonwealth of Australia and the state of Queensland, signed in March 2022.
** Statewide branch projects include initiatives to improve workforce capability and sustainability, delivering digital capability and digitally enabled treatment, care and support, and strengthening quality to reduce harm and improve outcomes.
Compiled by the Queensland Audit Office based on information from Queensland Treasury and the Department of Health.

| Work in progress Queensland Treasury started a project to improve how it manages levy funding in 2025. In consultation with relevant stakeholders including the Department of Health, Queensland Treasury is planning to define the scope of the levy’s use and set clear guidelines for its use. This is a positive step towards addressing several of the gaps we found. |
There is no coordinated approach to planning which services and infrastructure are funded.
There is no coordinated approach to planning how funding should be allocated across the continuum of care in line with government priorities and the levy’s intended purposes. Levy funding has been allocated in response to entity requests and has not been informed by whole-of-levy planning.
Many entities manage and deliver services across distinct parts of the continuum of care. Some entities have undertaken planning for their requests for levy funding and initiatives. This includes the Department of Health, which is responsible for planning and managing levy funding for specialised MHAOD services, which is discussed in Chapter 5. However, there is no whole-of-levy perspective across requests and initiatives to consider their expected contribution to intended outcomes.
Without a coordinated approach and responsibility for planning how funding should be allocated, responsible entities do not know whether the levy is going to the right services across the continuum of care.
Not all levy funding is monitored to understand whether it is achieving its intended purposes
No entity has oversight of how all levy funding is being spent or whether funded initiatives are contributing to intended outcomes. While Queensland Treasury tracks how much funding entities spend, its role does not involve checking how they spend their allocated funding.
Entities that receive levy funding are accountable for spending it for its approved use and for monitoring the performance and outcomes of their funded initiatives. The Department of Health has started to evaluate the performance of some of its levy-funded programs. However, responsibility for overseeing this information across all levy funded entities and initiatives has not been assigned.
This means there is no understanding of the impact of the levy as a whole, which is a significant investment in the MHAOD system. This information should inform future planning for how levy funds are invested to achieve intended purposes.
Without responsibility for the levy’s oversight, responsible entities do not know if the levy is:
- being used appropriately
- making the most of its substantial investment.
Recommendation 1 We recommend that Queensland Treasury consults with key entities to establish governance of the levy as a whole by:
|
Queensland Treasury can improve its processes to administer levy funding
Queensland Treasury tracks levy revenue and allocations, but does not have oversight of all expenditure
Queensland Treasury has a good understanding of how much levy funding is available at any time. It collects monthly data on levy revenue and tracks approved levy allocations.
However, it does not have accurate data about how much allocated levy funding has been spent by all entities. While entities report a high-level summary of their expenditure of levy funding to Queensland Treasury each year, some funding was allocated to the Department of Health to further allocate to other government departments. Queensland Treasury does not track how these funds are spent, and the Department of Health does not have the authority to track this expenditure.
There are other gaps in Queensland Treasury’s approach to administering levy funding
Queensland Treasury is responsible for providing advice on funding requests, and overseeing entity expenditure and requests for deferrals. At times, entities ask Queensland Treasury if they can defer their funding for a period of time to a future year. This means they can keep the funding but have more time to spend it. This is called a deferral.
Queensland Treasury could improve its advice, guidance, and oversight for levy deferrals. Any improvements should be considered within Queensland Treasury’s broader approach to managing funding and deferral requests. Figure 4C below details limitations of Queensland Treasury’s current approach to deferrals and the potential risks associated with those limitations.
Queensland Treasury: | This means that: |
|---|---|
| asks entities to provide information about why they want to defer unspent funding to future years. However, it does not always receive this. | Queensland Treasury does not always have sufficient information to understand why an agency needs a deferral, or if it is appropriate. |
| does not document its rationale for approving deferral requests. | it is not clear why Queensland Treasury approved all deferral requests we reviewed, or whether they were appropriate. |
| cannot identify when funding for individual initiatives is deferred multiple times. | funding could remain with entities instead of returning to Queensland Treasury for potential reallocation to other initiatives. |
does not always include its analysis about the levy in its written advice to the Cabinet Budget Review Committee. This includes information about:
| there is an increased risk of decision makers not receiving the information they need to allocate levy funding. |
has a manual system for tracking levy expenditure. It does not have an easy way to identify levy expenditure in agency reporting. Staff must rely on their knowledge of which entities and programs were funded from the levy to find this information. Further, Queensland Treasury has not documented its processes to manage levy funding. | if current staff leave, Queensland Treasury risks not being able to maintain this process or efficiently track levy expenditure. |
| has not defined a criteria or threshold for when it can approve requests to defer or change how funding is used, and when to escalate to the Cabinet Budget Review Committee for a decision. This is important because the levy is a special purpose fund that must be spent on initiatives that align with its legislation. | without clear criteria, Queensland Treasury could approve some deferral or change requests that should go back to the Cabinet Budget Review Committee for approval. |
| has not established funding conditions for entities, including decision making rights and tolerances for changes to cost, timing, scope, risk, quality and outcomes. | there is an increased risk that entities will make decisions about levy-funded initiatives that should return to the Cabinet Budget Review Committee. |
Compiled by the Queensland Audit Office based on information from Queensland Treasury.
Recommendation 2 We recommend that Queensland Treasury implements an internal policy for how it administers the levy. The policy should outline:
|
Recommendation 3 We recommend that Queensland Treasury provides guidelines to entities who receive levy funding, which at a minimum include:
|
Is the levy achieving its intended purposes?
The levy was intended to grow services and increase expenditure to reform Queensland’s MHAOD system. Funding has been allocated to a range of services and initiatives. However, the gap in planning, oversight, and outcomes for the levy as a whole reduces visibility of whether it is achieving its intended purposes.
The levy has committed more funding to expand and enhance mental health, alcohol and other drugs services
As Figure 4D shows, the levy has funded diverse MHAOD services and initiatives since it was introduced. This includes funding to hospital and health services (HHSs), non-government organisations (NGOs), and other government entities.
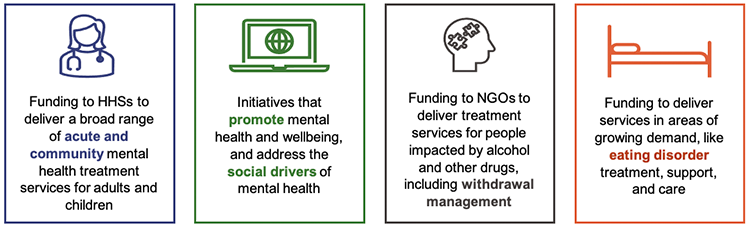
Compiled by the Queensland Audit Office based on information from the Department of Health and Queensland Treasury.
Through the levy, the Queensland Government has allocated $1.9 billion in operating funding to Better Care Together over 5 years. The Department of Health’s former plan for MHAOD services, Connecting care to recovery 2016–2021, received $358 million over 5 years.
$358 million funding invested in MHAOD services under Connecting care to recovery 2016–2021, in addition to existing core funding
$1.9 billion levy funding invested in MHAOD services from 2022–23 to 2026–27 under Better Care Together, in addition to existing core funding
Additional levy revenue invested in initiatives delivered by other government entities
Compiled by the Queensland Audit Office based on information from the Department of Health.
This increase in funding is to address an observation about Queensland’s historically low investment in MHAOD services from the Mental Health Select Committee’s inquiry. However, not all allocated funding for Better Care Together has been spent to date and some of this has been used to replace core funding for initiatives.
The levy has replaced existing funding sources for some initiatives
More funding has been allocated to MHAOD services, but the levy has also replaced existing funding sources for 4 initiatives delivered by Queensland Health, totalling $16.57 million each year.
One of the levy’s intended purposes is to increase funding and expenditure in the MHAOD system. The extent to which the levy was intended to increase MHAOD expenditure was not specified at the time the levy was introduced. If entities use the levy to replace existing funding sources, they can repurpose the base funding for other MHAOD initiatives, which would create a net increase in expenditure. However, this funding could also be repurposed for initiatives that are not related to MHAOD. Such initiatives may not contribute to the levy’s intended purposes of increasing MHAOD expenditure, and enhancing or reforming existing services.
Current data and reporting do not identify whether the levy has increased net expenditure across the MHAOD system.
Reporting about the levy is not transparent
There is not an entity monitoring and reporting on the levy’s allocations, expenditure, and performance as a whole. This is important to ensure confidence, accountability, and defensibility for the use of these significant amounts of public funds.
While there is some public reporting about the levy, it does not provide a complete or accurate view of the levy’s use across the MHAOD system, as Figure 4F shows.
What is reported? | 
| What is not reported? |
The Department of Health’s Better Care Together annual updates provide a summary of how the Department of Health’s largest funding allocation has been used across priority areas. This includes information on outputs. | The Department of Health did not publish an update in 2024–25. Previous updates did not report on progress towards achieving outcomes. The update does not capture all of the Department of Health’s levy allocations. | |
| Government agency annual reports and the budget papers report the levy’s actual and projected revenue. | 
| These do not include levy allocations, expenditure, or performance. |
| The Australian Institute of Health and Wellbeing (AIHW) reports expenditure on specialised MHAOD services by state and territory. The Department of Health has quality data on specialised services and reports this to the AIHW. | 
| This is not levy-specific. This does not provide timely expenditure information due to a lag between data collection and publication. |
Compiled by the Queensland Audit Office based on publicly available information.
The levy has a prescribed use under its legislation. Public reporting should enable parliament, the public, and businesses that pay the levy to understand:
- how these funds are spent
- whether the levy is achieving its intended outcomes.
5. Using the Department of Health’s levy allocation to deliver outcomes
This chapter focuses on how effectively the Department of Health has managed its allocation of the mental health levy. We focus on the Department of Health because it is the largest recipient of levy funding. It is also responsible for allocating some of its funds to other entities.
The Department of Health was allocated approximately 92 per cent of levy revenue from 2022–23 to 2026–27 to deliver:
- Better Care Together: A plan for Queensland’s state-funded mental health, alcohol and other drug services to 2027 (Better Care Together)
- 2 initiatives under the Queensland Women and Girls’ Health Strategy 2032 (Women and Girls’ Strategy) that relate to mental health and wellbeing
- the mental health part of disaster recovery initiatives
- further funding to entities outside the specialised mental health, alcohol and other drugs (MHAOD) service system to implement other initiatives.
The Department of Health further allocates levy funding to other entities to deliver initiatives and services. Entities include hospital and health services (HHSs), non-government organisations (NGOs), and other government entities.
The Department of Health is responsible for managing the performance and expenditure of its levy‑funded programs within the specialised MHAOD service system. Under the current levy governance structure, the Department of Health has not been given responsibility for:
- managing the performance of the levy as a whole
- overseeing how other government entities use the funding it allocates to them.
Is the levy contributing to outcomes for specialised mental health, alcohol and other drugs services?
The Department of Health’s levy funding has contributed to increases in key MHAOD outputs, such as expenditure, beds, and staff. The Department of Health does not yet know whether the levy is contributing to intended outcomes for the specialised MHAOD service system. This is partially due to delays in its evaluation and gaps in its approach to measuring performance across all programs. However, improvements to some health and wellbeing outcomes may only be evident in the longer term.
Outputs are the results or delivery of a specific activity or initiative. They can often be measured as a plan progresses and support the achievement of outcomes.
Outcomes refer to the impact and value that outputs create. They are often visible over the longer term.
The levy has contributed to increased expenditure, beds, and staff for specialised MHAOD services
The Department of Health has used its levy funding to support initiatives focused on increasing services, beds, and full-time equivalent (FTE) staff within Queensland’s specialised service system. For example, this includes funding to:
- HHSs to employ additional psychiatrists and operate new acute mental health beds in hospitals
- NGOs to grow investment in perinatal mental health community services.
The levy has contributed to an increase in expenditure, beds, and FTE staff for specialised MHAOD services since it was introduced. However, we cannot quantify the extent of this impact because the data also reflects other sources of funding.
Expenditure
The levy has contributed to increased expenditure on specialised MHAOD services in Queensland. For example, the Department of Health has spent over $120 million of its levy funding on initiatives that respond to mental health crisis and suicidality under Better Care Together from 2022–23 to 2024–25. This priority area aligns with the specialised services category.
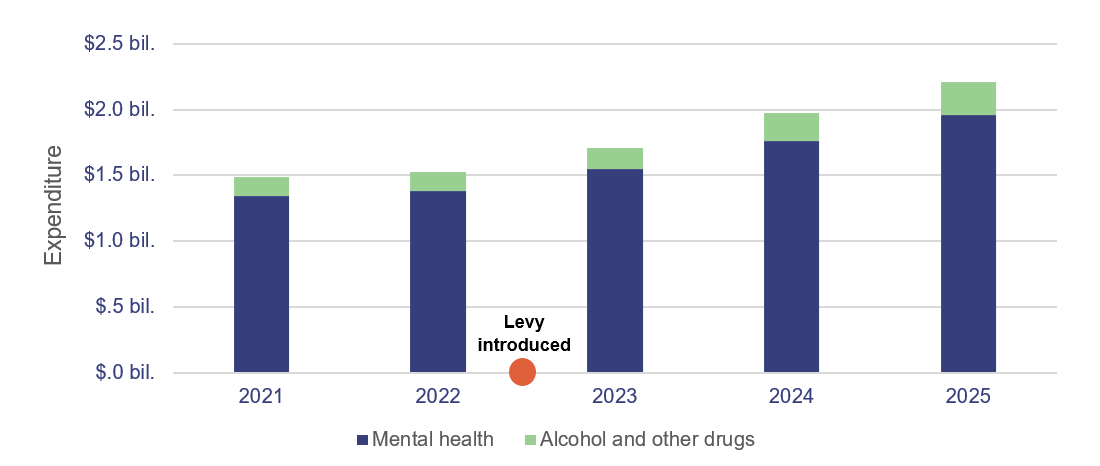
Note: The data only covers recurrent expenditure.
Compiled by the Queensland Audit Office based on data from the Department of Health.
Beds
Figure 5B shows that the number of available public beds and bed alternatives for specialised MHAOD services has increased since 2020–21. Bed alternatives are other furniture that provide accommodation for admitted patients, such as trolleys or cots.
The rate of change for MHAOD beds has also increased since 2022–23, when the levy was introduced. The Department of Health has used Better Care Together funding to deliver beds in several HHSs across the state. These include specialised beds for mothers and babies, and acute mental health beds for adults and adolescents.
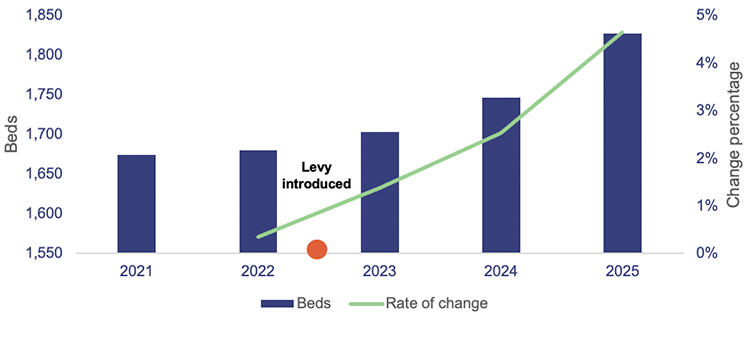
Compiled by the Queensland Audit Office based on data from the Department of Health.
Full-time equivalent staff numbers
The levy has funded 1,009 new FTE staff from 2022–23 to 2024–25. This is about 89 per cent of the total FTE staff the Department of Health intended to appoint under its Better Care Together plan during this period. The Department of Health has spent about $11.5 million of its levy funding to support initiatives targeted at growing and retaining the MHAOD workforce.
Queensland is experiencing well-documented challenges in maintaining its health workforce. Workforce growth has not kept pace with population growth, demographic changes, and increasing demand for healthcare. This affects the Department of Health and HHSs’ ability to recruit and retain qualified staff to new positions.
Figure 5C shows the increase in FTE staff for specialised MHAOD services from 2022–23 to 2024–25.
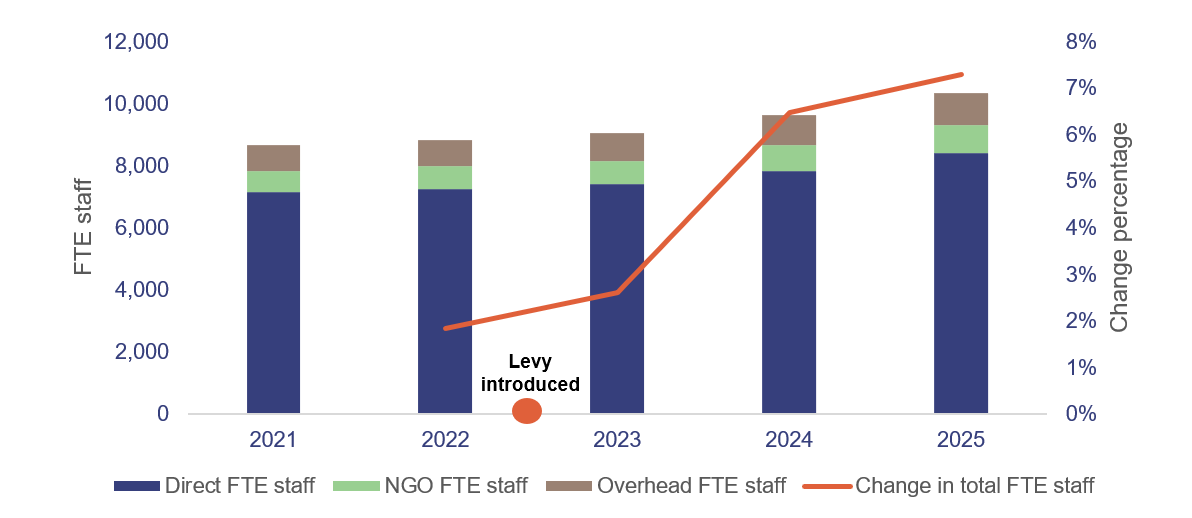
Compiled by the Queensland Audit Office based on data from the Department of Health.
The Department of Health has spent most of its levy funding
Most of the Department of Health’s levy funding is used to deliver Better Care Together. The Department of Health tracks how much funding is spent by HHSs, NGOs, and the Department of Health’s administrative and non-clinical units under this plan.
The Department of Health reports that it spent 89 per cent of its levy funding for Better Care Together in its first 3 years
The Department of Health reports it has spent approximately $705 million of its allocation of levy funding for Better Care Together from 2022–23 to 2024–25. This is 89 per cent of its allocation for this period. Figure 5D shows this expenditure by entity.
Other government entities that receive levy funding from the Department of Health are not required to report on their expenditure of this funding to Queensland Treasury. Instead, the Department of Health reports the funds as spent at the time it transfers them. This means that data on levy expenditure may not fully reflect the funds spent.
In addition, the Department of Health did not always make entities aware of the source of the funding or the levy’s prescribed use. This creates a risk that other government entities are not using the allocated funding for intended and approved purposes.
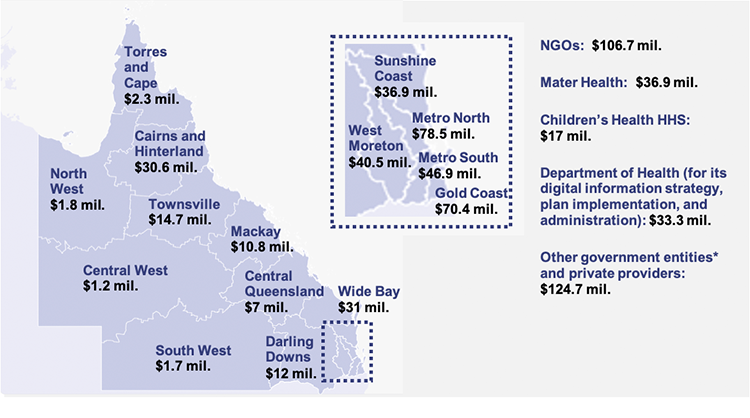
Note: * The Department of Health does not track actual expenditure by other government entities, which include the Department of Housing and Public Works, the Queensland Mental Health Commission, the Department of Youth Justice and Victim Support, Health and Wellbeing Queensland, and the Department of Trade, Employment and Training. This graphic shows the committed expenditure for these entities.
Compiled by the Queensland Audit Office based on data from the Department of Health as at June 2025.
Figure C2 in Appendix C shows a breakdown of expenditure by priority area under Better Care Together.
The Department of Health has deferred some of its levy funding under Better Care Together to future years
The Department of Health has not used all of the funding allocated for the Better Care Together plan to date.
Figure 5E shows that the Department of Health deferred $93.6 million in operational funding and $120.5 million in capital funding for Better Care Together in 2024–25. This means it did not spend all of its allocated funding for 2024–25 and transferred the underspend to a future year.
The Department of Health has investigated the causes of underspends within individual initiatives, and shares these learnings across the Better Care Together program. The causes include challenges in recruiting and retaining Queensland’s health workforce and delivering infrastructure.
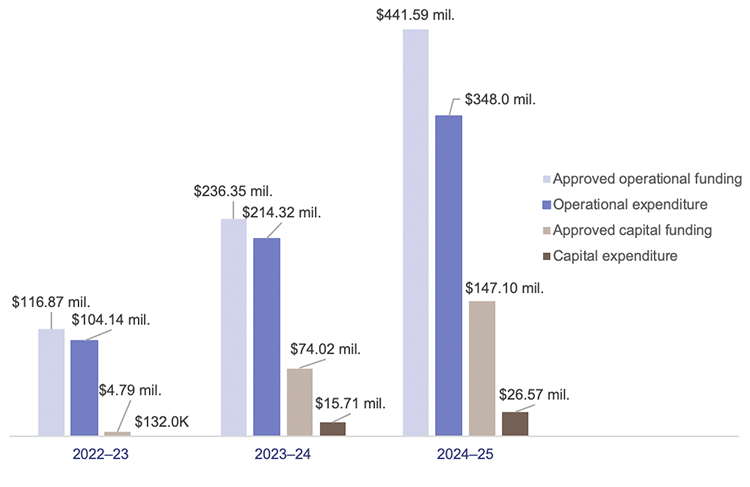
Note: Funding and expenditure for 2022–23 covers the period from the levy’s introduction on 1 January 2023 to 30 June 2023. The capital funding figures include a provision for capital of $65 mil. for 2023–24 and 2024–25. This funding may be returned to operational expenditure if required.
Compiled by the Queensland Audit Office based on data from Queensland Treasury and the Department of Health.
The Department of Health does not yet know if its programs are contributing to outcomes
The Department of Health engaged an external consultant to develop an evaluation framework for Better Care Together. Its framework includes performance indicators, outputs, and outcomes. It could improve its framework to better understand the impact of its plan and drive continuous improvement, noting that some outcomes may only be realised in the longer term.
The Department of Health finalised its evaluation framework for Better Care Together in August 2024, which was during year 3 of the 5-year plan.
We found that: | This means that the Department of Health cannot: |
|---|---|
| the Department of Health planned to collect baseline data and do a formative evaluation in early 2025, but this had not been completed at the time of the audit. | use insights from the evaluation to make timely adjustments to the plan. |
the Department of Health did not provide quantitative data to its evaluator to inform the formative evaluation of Better Care Together. The Department of Health advised that this is because it could not grant the evaluator’s data access request in time. This data is a relevant source for several indicators in the evaluation framework. | represent a complete view of the Better Care Together plan’s progress towards achieving outcomes in its formative evaluation. The Department of Health plans to include this data in the next phase of its evaluation. |
| the evaluation framework does not include any economic criteria. | measure whether the program is generating a return on investment. |
| the evaluation framework specifically excludes assessment of the outcome of improved mental health and wellbeing. The framework notes this is because there is no standardised measure of individual wellbeing and it is difficult to attribute changes in this outcome to the plan. | conclude on whether Better Care Together has achieved one of its intended outcomes of improving mental health and wellbeing. |
Compiled by the Queensland Audit Office based on information from the Department of Health.
Is the Department of Health effectively managing its allocation of levy funding?
The Department of Health is effectively managing its largest allocation of levy funding for Better Care Together. However, it can improve how it governs all of its levy-funded programs and how it contributes to whole-of-levy planning.
The Department of Health has developed processes to manage most expenditure, but should implement a risk-based approach
The Department of Health manages levy funding differently across key programs and entities. A positive example is its design and implementation of Better Care Together funding assurance processes for HHSs. This involves controls to support the appropriate release and expenditure of funding as shown in the case study below.
Managing HHS expenditure under Better Care Together |
|---|
The Department of Health has designed processes to release levy funding to HHSs and oversee how they spend it under Better Care Together. The Department of Health requires HHSs to complete an initiative assurance statement to receive funding. This statement provides the Department of Health with visibility of whether the HHS has started the initiative or hired relevant staff. This statement is endorsed by the Executive Director of the relevant Department of Health branch before funding is released. HHSs have 4 opportunities each year to submit these statements for new initiatives within Better Care Together. The Department of Health also requires HHSs to report back on how they spent the levy funds on an annual basis. This includes a detailed summary of expenditure against their allocation, which is supported by a general ledger extract. Chief Financial Officers at each HHS are required to certify this information. If the HHS has not spent its full allocation, the Department of Health takes back unspent funding. The Department of Health must request a deferral of the underspend across its full allocation of levy funding from Queensland Treasury each year. These processes help the Department of Health oversee whether HHSs spend funds on approved initiatives. 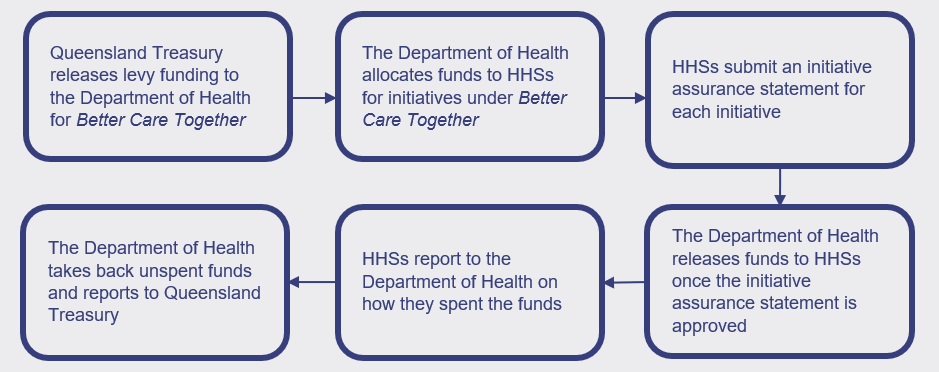
|
Compiled by the Queensland Audit Office based on information from the Department of Health.
These processes provide oversight for the Department of Health, but they are time and labour intensive for HHSs. The Department of Health has not yet set up a risk-based approach to make financial and performance monitoring less time-consuming as the initiatives become business as usual. Adjusting monitoring and reporting requirements would reduce the resourcing impact on HHSs while ensuring the Department of Health retains oversight of its allocation of funding.
The Department of Health can improve its governance for future programs
The Department of Health has not established a coordinated approach to governing its full allocation of levy funding. For example, initiatives that received funding under the Women and Girls’ Strategy do not have the same monitoring or reporting arrangements as Better Care Together initiatives.
This makes it more difficult for the Department of Health to consistently measure outcomes and assess the impact of its full allocation of levy funding.
The Department of Health implemented a governance structure for its investment under Better Care Together, but there are gaps that reduce its effectiveness.
The Department of Health: | But: |
|---|---|
| established an assurance committee for Better Care Together. This committee has a role in providing advice to inform decisions to reallocate funding. | this committee made decisions to reallocate Better Care Together funding, which did not align with its role of providing advice on these matters. It also did not regularly discuss or escalate key risks, which was one of its responsibilities. |
| includes diverse membership in its assurance committee, including from the community sector and HHSs. This has led to robust discussion. | because the committee has a role in assuring the release and acquittal of funding, it may not be the right forum to obtain stakeholder perspectives. |
| has performance outputs and indicators for Better Care Together. | it is not regularly monitoring or reporting on performance against these outputs or indicators. Those charged with governance for the program may not always receive complete information to inform their decisions. |
Compiled by the Queensland Audit Office based on information from the Department of Health.
Recommendation 4 We recommend that the Department of Health improves how it governs all its allocations of levy funding by establishing:
|
The Department of Health effectively plans investment in services, but could enhance its approach
The Department of Health has allocated its levy funding to HHSs, NGOs, and other government entities, but could enhance its approach to planning this investment.
Currently, the Department of Health adapts outputs from the National Mental Health Service Planning Framework and its own Queensland Drug and Alcohol Service Model to determine demand for MHAOD services. The Department of Health then consults with stakeholders including HHSs about the outputs from its planning process.
This approach meets national requirements.
Stakeholders have provided feedback that Better Care Together priorities do not fully address their needs, and it is difficult to adjust the funding they receive to meet emerging priorities. This is supported by progress monitoring information and expenditure data.
Including input on unmet regional demand and operational contexts could improve the effectiveness of service planning and costing of initiatives.
MHAOD planning would then incorporate differing needs across HHSs including regional demand, service availability, and workforce information.
The Department of Health could also incorporate a continuous service planning approach across the 5‑year plan to ensure that changes to populations, demographics, and supply and demand for particular services are included.
Recommendation 5 We recommend that the Department of Health informs planning for whole-of-levy investment by progressing and enhancing its:
|