
Overview
There is no greater responsibility of government than protecting vulnerable children. It unquestionably requires constant commitment, vigilance, and agility, and seamless integration and cooperation across government and non-government service providers. Ensuring vulnerable children are quickly sighted and their safety established must be the priority of all governments.
Tabled 4 August 2020.


Auditor-General’s foreword
There is no greater responsibility of government than protecting vulnerable children. It unquestionably requires constant commitment, vigilance, and agility, and seamless integration and cooperation across government and non-government service providers. Ensuring vulnerable children are quickly sighted and their safety established must be the priority of all governments.
In this audit we found that staff and agencies across the family support and child protection system are committed to improving the system and much has been achieved in recent years. But despite their commitment and achievements, the system is not perfect, and much work still needs to be done.
We found a system under pressure from high demand, and one that is not adequately structured to meet the complex, 24/7 needs of vulnerable children.
Child death reviews consistently highlight the need for decisive, seamless, and coordinated communication, decision-making, and action across public sector entities and non-government service providers.
In this report, I provide detail on my audit findings, insights and recommendations for improvement.
I also note the expected significant economic and social impacts of the COVID-19 pandemic. These impacts are likely to affect employment services, housing, domestic and family violence services, child protection, mental health, and substance abuse support services. This will place ever greater demand on Queensland’s family support and child protection system, further increasing the need for the community, public sector and non-government service providers to act collectively to ensure no child falls through the gaps.
Brendan Worrall
Auditor-General
Report on a page
This audit assessed how effectively Queensland public sector entities work together for the safety and wellbeing of Queensland children. We audited six public sector entities responsible for delivering family support and child protection services to determine whether:
- Queensland’s family support and child protection system is managed to ensure efficient and effective coordination across agencies
- Queensland government agencies share responsibility for the continuous improvement of the family support and child protection system.
Progress has been made but the system is still under pressure
Entities have made good progress implementing recommendations from reviews over recent years and reforming the family support and child protection system. In most cases, agencies cooperate well, but this can be further enhanced. However, the system remains under pressure from high demand and the growth in families with multiple and complex needs. The social and economic impacts of the COVID-19 pandemic are likely to add further pressure to the system and agencies need to be prepared.
Early support is important but greater capacity is needed
Vulnerable families have greater support available to them now than previously and more report that the support is meeting their needs. Increasing the rates of consent by families in need of support would be likely to provide further benefits (at present half the families referred to family support services consent to receiving support). Improving the number of families engaging in these services would be likely to strengthen Queensland communities and reduce the pressure on the system. But at present, family support services do not have the capacity to provide significantly more services.
Enhancing the shared approach to child protection reports is needed
Demand on the child protection system remains high. The Department of Child Safety, Youth and Women (Department of Child Safety) is generally quick to prioritise and investigate reports that indicate a child is in immediate danger but could improve timeliness for reports assessed as less urgent. Entities need to progress development of a multi-disciplinary intake process to integrate information from all relevant agencies, including non-government organisations, and to facilitate a shared responsibility for triaging and responding to all child harm reports.
The Department of Child Safety is finding it increasingly difficult to place children into care based on their needs. A shortage of carers and children staying in care longer are contributing to this challenge. Consequently, some children are placed into out-of-home care based on what is available rather than what matches their specific needs.
Audit recommendations
We made nine recommendations to improve the family support and child protection system.
Introduction
Protecting the rights and managing the safety of Queensland children is a responsibility shared across government and the broader community. Government, non-government organisations, and communities work together to deliver services to families that need support caring for children. In Queensland, the family support and child protection system (the system) operates in two key areas: early intervention to support families, and protection of children at risk of significant harm without a parent able and willing to protect them from the harm (including those needing out-of-home care).
The growth in families with multiple and complex needs is placing greater pressure on the system. The prevalence of poverty, mental illness, substance abuse, incarceration rates, and domestic violence in families are all contributors. These challenges are not unique to Queensland and are well recognised both nationally and internationally. There is some early evidence to suggest these issues will be exacerbated by the significant economic and social impacts of the COVID-19 pandemic. The high percentage of children with a disability who are in care and the over-representation of Indigenous children in the system are indicators of specific challenges.
The objective of this audit was to assess how effectively Queensland government agencies work together for the safety and wellbeing of Queensland children. As part of this audit, we assessed family support services and the child protection system. Appendix B contains further details about the audit scope and our methods.
Reforms to Queensland's family support and child protection system
In 2013, the Queensland Child Protection Commission of Inquiry (Carmody Inquiry) recommended major reforms to the system. It provided a program for reforming the system over a 10-year period to:
- reduce the number of children in the child protection system
- revitalise child protection frontline services and family support to break the intergenerational cycle of abuse and neglect
- refocus oversight on learning, improving, and taking responsibility.
Since 2013, key reform activities have included:
- new support services for families (94 non-government organisations across Queensland)
- establishing and restructuring statutory bodies to oversee the system and protect the rights of children
- providing for greater information sharing between entities resulting from amendments to the Child Protection Act 1999 in July 2017 and the development of new guidelines
- mandatory reporting requirements expanded to early childhood.
The Queensland Government is now halfway through the reform program. It has designed, developed, and implemented a series of reforms and is now reviewing and, where necessary, adjusting elements. As at 30 June 2019, the Department of the Premier and Cabinet reported that 107 of the 121 recommendations from the Carmody Inquiry have been delivered, and the remaining 14 are underway.
Since the Carmody Inquiry, several system reviews, inquiries, and the Royal Commission into Institutional Responses to Child Sexual Abuse have added further recommendations aimed at improving the system. An additional 12 reviews and evaluations of the system or a component of the system have occurred since 2013–14.
These reviews have resulted in 612 recommendations to entities within the system. Entities continue to implement these recommendations.
Appendix D shows the 12 reviews and evaluations. It excludes entities' smaller, internally focused reviews and evaluations.
Who delivers family support and child protection services?
A range of government and non-government entities deliver family support and child protection services. These include:
Department of Child Safety, Youth and Women
The Department of Child Safety, Youth and Women (Department of Child Safety) is Queensland's lead agency for child safety and adoption services. It has a statutory obligation to protect children and young people who have been harmed or are at risk of harm, and whose parents are unable or unwilling to protect them. It delivers these services across five Queensland regions: south east, south west, northern, Moreton, and central. Appendix E provides details of the five regions.
Queensland Family and Child Commission
The Queensland Family and Child Commission (the Commission) was established on 1 July 2014 as a result of the Queensland Government's response to the Carmody Inquiry. Under the Family and Child Commission Act 2014, it has an oversight role. Its purpose is to:
- promote the safety, wellbeing, and best interests of children and young people
- promote and advocate for the responsibility of families and communities to protect and care for children and young people
- improve the child protection system.
Other public sector entities
Several other public sector entities have specific responsibilities to identify and report harm to children under the Child Protection Act 1999 and other relevant legislation. These include:
- Queensland Police Service
- Department of Education, including under the Education (General Provisions) Act 2006
- Queensland Health.
The Office of the Public Guardian also plays a key role in promoting and protecting the rights and interests of children and young people in the child protection system by performing child advocacy functions, including visiting children in out-of-home care.
The Department of the Premier and Cabinet was responsible for leading the Carmody Inquiry reforms.
The Office of the Director of Child Protection Litigation, within the Department of Justice and Attorney-General, also plays a key role in the system and is responsible for child protection proceedings in the Children’s Court of Queensland.
Non-government organisations
In January 2015, the Department of Child Safety introduced family support services in response to recommendations from the Carmody Inquiry. The Carmody Inquiry found that Queensland had under-invested in family support programs compared with other jurisdictions.
The intent of family support services is to provide early support (such as anger-management or alcohol and drug support) to vulnerable families, to prevent harm from occurring and reduce the number of children coming into the child protection system.
Since January 2015, the Department of Child Safety has funded 94 non-government organisations to provide support to families across the state. Family support services can only be provided to families that consent to the service. Three types of family support services are available:
- Family and Child Connect services—which connect families to a support service that suits their needs
- Intensive Family Support services—which deliver a range of services, including case management support to families with multiple and complex needs
- Aboriginal and Torres Strait Islander Family Wellbeing services—which provide specialist support for Indigenous families with multiple and complex needs.
Government organisations, non-government organisations, and the general community can refer families requiring support to Family and Child Connect services, with the consent of the family. Government agencies and non-government service providers who are prescribed entities can also refer families to family support services without the family's consent. The Department of Child Safety may refer the reports it receives that do not meet the threshold of significant harm if it decides the family would benefit from additional support.
How is harm or risk of harm to a child reported?
Any person who suspects that a child may be in need of protection, or an unborn child may be in need of protection after birth, can make a report to the Department of Child Safety.
Under the Child Protection Act 1999 (the Act) a child who is in need of protection:
- has suffered significant harm, is suffering significant harm, or is at unacceptable risk of suffering significant harm; and
- does not have a parent able and willing to protect the child from the harm.
The Act defines harm to a child as 'any detrimental effect of a significant nature on the child's physical, psychological or emotional wellbeing'.
The Act requires certain professionals (called mandatory reporters) to make a report to the Department of Child Safety if they suspect a child is in need of protection. Mandatory reporters are:
- teachers
- doctors
- registered nurses
- police officers with child protection responsibilities
- a person performing a child advocate function under the Public Guardian Act 2014
- early childhood education and care professionals, from 1 July 2017.
Queensland's system has two reporting pathways. A person can either:
- report their concerns about a child's safety to the Department of Child Safety if they suspect a child is in need of protection
- refer concerns about a child (that is, where they suspect the child is not in need of protection and the family could benefit from additional support and assistance) to family support services, with the family's consent. Government agencies and non-government service providers who are prescribed entities can refer a family without their consent. Entities refer to concerns referred to family support services as ‘child concern reports’.
Figure A shows the two reporting pathways for concerns about a child's safety.
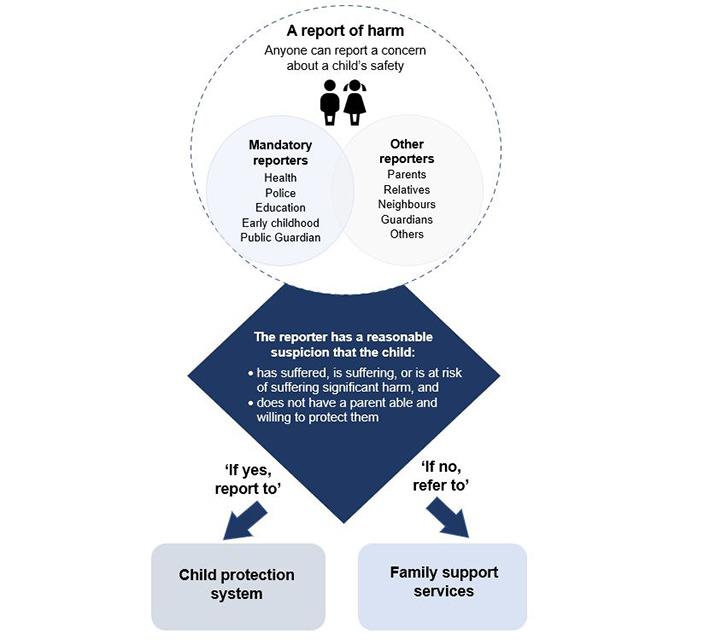
Queensland Audit Office.
The Department of Child Safety has placed child safety officers within Family and Child Connect services to identify children referred to family support services that should have been reported to the Department of Child Safety and to redirect them to the Department of Child Safety for investigation.
What happens when alleged harm or risk of harm to a child is reported?
Screening reports of child harm
The Department of Child Safety regional intake services receive concerns about child safety from professionals, family members, and the public. Intake service staff screen reports of harm or risk of harm to determine whether the allegations meet the threshold for an investigation (that is, a child has suffered, is suffering, or is at unacceptable risk of suffering significant harm and does not have a parent able and willing to protect them from harm). The Department of Child Safety can refer reports that do not meet the threshold for investigation to family support services. Throughout this report we refer to all reports of alleged harm or risk of harm that the Department of Child Safety receives as ‘child harm reports’.
Investigating reports of child harm
The Department of Child Safety’s child safety officers are responsible for investigating allegations where they reasonably suspect a child is in need of protection. Staff record all information about a child's safety in the Department of Child Safety’s Integrated Client Management System.
The Queensland Police Service also investigates reports of child harm that are of a criminal nature and works in partnership with the Department of Child Safety when an investigation requires a joint response.
Placing children into care
The Department of Child Safety has several options for children requiring ongoing care and protection. Where appropriate, its preferred option is to keep a child with their immediate or extended family and provide support to the family to protect the child. In some instances, the Department of Child Safety will need to remove a child from their home and place them into out-of-home care, either with extended family, with foster carers, or in residential care.
Summary of audit findings
Supporting families early
Vulnerable families have greater support available to them now than they did before the 2013 Queensland Child Protection Commission of Inquiry (Carmody Inquiry). In addition, more families now report that family support services are meeting their needs. Currently, only half the families referred to family support services consent to receiving support. Some support agencies make limited attempts to contact families and experience delays in making contact; this may influence whether families consent to receiving support. The Department of Child Safety, Youth and Women (Department of Child Safety) needs to work with family support service providers to increase engagement with families, particularly those providers with low consent rates. However, even if they are successful in increasing consent rates, the current system is unlikely to have the capacity to meet increased demand. We heard from some family support service providers who reported high caseloads and said they were struggling to keep up with demand. We could not assess their caseloads because they do not record this information.
The COVID-19 pandemic is expected to have significant social and economic impacts that will adversely affect some Queensland families. This is likely to increase demand on the family support and child protection system. The Queensland Government is anticipating an increase in demand for domestic and family violence services arising from COVID-19. In April 2020, it announced it would provide an additional $7.5 million to support domestic and family violence victims.
Improving the quality of data captured by family support service providers will enable the Department of Child Safety and the Queensland Family and Child Commission (the Commission) to more effectively assess the outcomes achieved by family support services for families experiencing vulnerability.
Protecting children from harm
Mandatory reporters make a large number of reports to the child protection system that do not meet the threshold for investigation (the Department of Education was the highest contributor of reports that did not meet the threshold for investigation). Some remain cautious about the ramifications of failing to report and are unwilling to share this risk.
The existing system is not structured to manage the volume of reports that are generated by this low-risk approach taken by some mandatory reporters. The Department of Child Safety and other entities have tried approaches, such as education to encourage mandatory reporters to report directly to family support service providers matters that are unlikely to meet the threshold for an investigation. Child harm reports that do not meet the threshold can nevertheless be useful in providing a cumulative assessment of harm to the child over time. A child death review highlighted the need to consider and assess cumulative harm to a child. Therefore, having appropriate systems and processes to better integrate and analyse information would allow for a more informed assessment of the child’s immediate safety.
The Department of Child Safety is quick to prioritise reports that indicate a child is in immediate danger and requires a 24-hour response. Between 2013–14 and 2018–19, the median time taken by child safety officers to sight a child who was in immediate danger and required a 24-hour response was 19 hours and 12 minutes—from the time the intake service received the child harm report. However, the Department of Child Safety is not timely in sighting children for child harm reports that are less urgent and require a five- or 10-day response. We found that regions with the highest staff turnover and the highest transfer of staff between regions also had the longest delays to sight a child.
Outside of standard business hours, the Department of Child Safety provides a limited after-hours intake, response, and support service. It has an after-hours service centre located in Brisbane, which is responsible for after-hours child protection matters in all regions across the state. Regional Department of Child Safety staff and Queensland police expressed concerns about the capacity and ability for the service centre to respond after hours. We were provided with examples of police having difficulty getting support from the after-hours service centre.
The Department of Child Safety is finding it increasingly difficult to place children into care based on their needs. There are a variety of factors contributing to this difficulty in placing children into care, including a shortage of carers and children staying in care longer. The shortage of carers is likely to be contributing to a higher number of placement changes. Between 2013–14 and 2018–19, 18 per cent of children placed into care by the Department of Child Safety had between six to 10 placements, six per cent had 11 to 20 placements, and 0.3 per cent had 21 to 30 placements.
Managing the system
Queensland's family support and child protection system has the appropriate governance vehicles and oversight in place to ensure the system is performing effectively. However, the role and purpose of the Interdepartmental Committee and the Department of Child Safety’s Regional Child, Youth and Family Committees could be better defined to strengthen the existing governance and oversight arrangements.
The Commission is providing oversight of the system and has helped to identify key issues and drive change across the system. Finalising its vulnerability project (identifying high risk areas) and its oversight strategy should help the Commission ensure it focuses on the most pressing system issues and give stakeholders greater visibility of its proposed program of work.
Both the Commission and the Department of Child Safety regularly monitor and report on the performance of Queensland's child protection system. The performance information is useful to child safety stakeholders and can help inform decision making across the system.
The Department of Child Safety could enhance its publicly reported performance data to more clearly report the time taken to commence an investigation. For example, its publicly reported data does not state that the time taken to commence investigating five- and 10-day priority reports is based on business days, not calendar days. Unless stated, readers of the department’s performance reports are naturally likely to assume the reported number of days to commence an investigation refers to elapsed calendar days. Reporting the time taken to commence an investigation based on calendar days or disclosing that the time is based on business days would provide transparent reporting and avoid readers misinterpreting the figures.
For the 2018–19 financial year, the Department of Child Safety reported that 92.5 per cent of its 24-hour priority investigations were commenced and the child was sighted within 24 hours. While this is accurate, it does not include the time taken to screen the child harm reports. When the screening and approval period is included, these investigations were commenced, and the child sighted, within four days of the Department of Child Safety receiving the child harm report.
In September 2019, the Department of Child Safety changed its measure of commencing an investigation for five- and 10-day priority reports from the time taken to sight a child to the time taken to gather new information. This change better aligns its practice with other states and territories. It will be important for the Department of Child Safety to monitor this change to ensure there is clarity and continued priority on verifying a child’s safety. As such, there is also value in the Department of Child Safety continuing to monitor the time taken to sight a child.
Audit conclusions
Following the various reviews and recommendations, the Queensland government entities with prime responsibility for the safety and wellbeing of Queensland children have improved how effectively they manage the system and work together. Entities have made good progress implementing recommendations from the Carmody Inquiry, and other reviews and evaluations. There have also been some significant system and process improvements.
That being said, the reforms have not achieved all the expected outcomes. The number of child harm reports continues to increase, staff struggle to find appropriate placement for children in need of care, and a high proportion of families do not receive the support services they need. Consequently, Queensland's family support and child protection system remains under considerable pressure and the entities need to do more to ensure they and non-government entities work effectively together. Effective partnerships will also be vital in the recovery phase of the COVID-19 pandemic, which is expected to have significant economic and social impacts. These impacts are likely to negatively impact employment, housing, domestic and family violence, child protection, mental health, and substance abuse.
Families continue to present with multiple and complex needs. While the Carmody Inquiry highlighted some of the key risk factors affecting families (for example domestic violence, mental health, and alcohol and substance abuse), their prevalence and impact were perhaps not as apparent as they are now. These factors can be exacerbated for children who come from families facing poverty or a history of incarceration. More effective leadership and governance across the system would help entities address these key risk factors to ensure families receive adequate support. More needs to be done to promote family support services, improve consent rates, and ensure there is sufficient capacity to support families in need.
The Department of Child Safety is struggling to cope with the number of reports it receives. Approximately 80 per cent (547,261) of the reports it received between 2013–14 and 2018–19 did not meet the threshold for investigation. Better education for mandatory reporters is necessary, but alone is unlikely to significantly change reporter behaviour. Under the current system, mandatory reporters (teachers, police, health workers) are expected to understand their reporting obligations and accurately interpret and apply legislation when determining whether they should report a concern to family support services or the child protection system. The agencies provide guidance to mandatory reporters and have additional controls to help mandatory reporters correctly report their concerns about child safety. Nevertheless, some mandatory reporters still feel they bear the legislative risk of incorrectly reporting. As such, they have not changed, and are unlikely to change, their reporting behaviour to the extent necessary to reduce the number of reports not meeting the threshold for significant harm.
Entities should consider evaluating the merits of establishing a multi-disciplinary intake process to efficiently and effectively triage all child harm reports. The intake process should integrate information from all relevant agencies, including non-government organisations, to facilitate a coordinated assessment, triage, and response to all child harm reports. This should enable improved decision making with greater access to more complete and accurate information when screening and investigating child harm reports. It is also likely to strengthen the sharing of responsibility across relevant public sector entities for identifying needs and keeping children safe.
Recommendations
Family support services data and reporting
We recommend that the Department of Child Safety, Youth and Women, in collaboration with family support services:
1. establish minimum service-level requirements based on better practice for engaging with families requiring support by Intensive Family Support and Aboriginal and Torres Strait Islander wellbeing services. It should tailor these requirements to the demographics of each region
2. collaborate with family support services to monitor outcomes and increase consent rates and the quality of data captured in the Advice, Referrals and Case Management database
3. automate the transfer of those child harm reports that do not meet the threshold for investigation but the family may benefit from family support services between the Integrated Client Management System and the Advice, Referrals and Case Management database.
Reporting alleged harm or risk of harm
We recommend that the Department of Child Safety, Youth and Women and entities with mandatory reporting responsibilities:
4. establish a multi-disciplinary intake process for efficiently and effectively triaging all child harm reports. The intake process should integrate information from all relevant agencies, including non-government organisations, to assess the cumulative risk and to facilitate a shared responsibility for triaging and responding to all child harm reports. This should prioritise the immediate safety of the child and not delay the Department of Child Safety, Youth and Women from immediately responding to a child harm report.
We recommend that the Department of Education:
5. provides greater support and training to principals and teachers to assist them in determining the appropriate pathway to report concerns about a child's safety.
Responding to alleged harm or risk of harm
We recommend that the Department of Child Safety, Youth and Women:
6. enhances its existing model for responding to alleged harm or risk of harm by:
- expanding its after-hours child safety protection services to ensure its child safety officers can better respond to child harm reports across the state in a timely manner
- providing adequate training, support and mentoring to child safety officers to enhance their decision-making skills, including an induction program for new staff.
Out-of-home care
We recommend that the Department of Child Safety, Youth and Women, in collaboration with the Queensland Family and Child Commission:
7. improve outcomes for children placed in out-of-home care. This includes:
- ensuring that children are placed in the most appropriate and stable type of care to meet their needs, rather than based on availability of care
- improving the quality and availability of out-of-home care options available to children requiring care
- reviewing the capability and capacity of carers, including the appropriateness of their experience, training, and qualifications
- reviewing the contracts of out-of-home care providers to ensure they include appropriate key performance indicators and clearly outline expectations
- identifying opportunities to increase the number of Indigenous children placed with kin, Indigenous communities, or Indigenous carers.
System governance
We recommend that the Department of Child Safety, Youth and Women and the Department of the Premier and Cabinet, in collaboration with other relevant public sector entities:
8. more clearly define the roles, purpose, and interrelationship of the Interdepartmental Committee and the Regional Child, Youth and Family Committees. This should include:
- expanding the role of the Interdepartmental Committee to provide greater leadership and strategic direction of the system
- ensuring the Interdepartmental Committee is working collaboratively with stakeholders and partners to resolve systemic issues and advance state and regional priorities, including through input from Regional Child, Youth and Family Committees.
We recommend that the Department of Child Safety, Youth and Women:
9. enhances its performance management by:
- internally reporting the time taken to gather information and sight a child for all investigations (24-hour, five-day, and 10-day investigations)
- more clearly defining the criteria for assessing the time taken to commence an investigation
- improving its publicly reported performance data by clearly identifying the basis of its measurements, including whether it is using business days or calendar days.
1. Supporting families early
Introduction
The Queensland Child Protection Commission of Inquiry (Carmody Inquiry) emphasised the importance of providing early support to vulnerable families to prevent harm from occurring or to minimise behaviour that leads to harm. The Carmody Inquiry proposed that providing greater support services and early intervention for families would provide better outcomes for families and reduce demand on the child protection system.
Following the Carmody Inquiry, the Queensland Government funded 94 non-government organisations to provide support to families across the state (collectively referred to as family support services). Family support services include:
- Family and Child Connect services—which connect families to a support service that suits their needs
- Intensive Family Support services—which deliver a range of services, including case management support to families with multiple and complex needs
- Aboriginal and Torres Strait Islander Family Wellbeing services—which provide specialist support for Indigenous families with multiple and complex needs.
Prior to the reform, families could still seek support from various organisations and initiatives, but there were fewer providers and there was often no formal link between providers and the child protection system.
In this chapter, we assess the provision of family support services to vulnerable families, including the techniques used and time taken to engage with families and the number of families that consent to receiving support.
The Department of Child Safety, Youth and Women (Department of Child Safety) started a staged approach to establishing the 94 family support service providers in January 2015. In June 2015, the Department of Child Safety implemented the Advice, Referrals and Case Management (ARC) database for family support providers to record information about vulnerable families and the support they provide.
Effectiveness of family support services
Vulnerable families now have greater support available to them than previously and more families that received services reported to family support services that their needs were met. Currently, only half the families referred to family support services consent to receiving support.
To be effective, public sector entities and family support services must:
- educate and communicate to mandatory reporters and the public about these services and how to access them
- engage well and quickly with families
- obtain consent to provide these services
- ensure the services deliver the support needed to prevent subsequent harm.
Figure 1A shows the number of cases referred to family support services by the Department of Child Safety, public sector entities, and other individuals between 2016–17 and 2018–19, and their status.
|
Status of cases |
Number of cases |
Percentage (%) |
|---|---|---|
|
Families either refused support, dropped out of contact, or could not be located |
36,736 |
54.5 |
|
Families were referred to another support service |
10,380 |
15.5 |
|
Families received support |
15,096 |
22.5 |
|
Cases remain open |
5,242 |
7.5 |
|
Total cases referred to family support services |
67,454 |
100 |
Notes: This excludes 11,204 cases where family support services were already providing support to the family or other categories that did not require a response from family support services.
Queensland Audit Office using ARC data provided by the Department of Child Safety.
The percentage of families that reported family support services fully met their needs increased from 82 per cent (3,726) in 2016–17 to 90 per cent (4,201) in 2018–19.
We do not know if some of the families who dropped out of contact or refused support did so because family support services were not meeting their needs. Further examination of why these families dropped out of contact may identify opportunities to improve the delivery of family support services.
Educating and communicating about family support services
Family support services receive referrals for families requiring support either directly from the family, from mandatory reporters and non-government organisations (direct referrals), or from the Department of Child Safety.
Public sector entities that have staff with mandatory reporting obligations could better inform their staff about the circumstances in which they could directly refer concerns about a child's safety to family support services. Between 2016–17 and 2018–19, 32,140 cases were reported to the Department of Child Safety that it subsequently assessed as not meeting the threshold for investigation and referred to family support services. This represents 48 per cent of all cases referred to family support services over this period.
The number of reports directly referred to family support services by mandatory reporting entities (as opposed to those referred by the Department of Child Safety) increased by 34 per cent from 5,823 in 2016–17 to 7,822 in 2018–19. This growth is positive, but it still has not reduced demand on the child protection system as anticipated by the Carmody Inquiry.
Since July 2016, the number of reports to the child protection system has increased by 12 per cent. Prior to the Carmody Inquiry, the Department of Child Safety forecast that growth in demand would increase more than it has. The reduced growth in demand may be due to the implementation of reform, including the introduction of family support services.
The implementation of family support services occurred in stages. In January 2015, the Department of Child Safety contracted 23 non-government organisations to provide support services to vulnerable families. It contracted an additional 38 family support providers in
2016–17 and 33 in 2017–18.
Since the introduction of family support services, there have been two marketing campaigns to promote family support services. Better education and awareness of family support services, for both mandatory reporters and the public, is necessary to further improve the number of direct referrals and alleviate pressure on the child protection system.
There is an unwillingness by entities engaging with children to refer a child to family support services in case the matter is more serious than first thought. As such, entities tend to report their concerns about a child's safety to the Department of Child Safety, rather than referring directly to family support services. Figure A (in the introduction of this report) describes the two reporting options available. We discuss the behaviour of those responsible for reporting harm (referred to as mandatory reporters) further in chapter two.
Obtaining consent from families
The effectiveness of family support services is dependent on families consenting to receive support. Currently, half the families referred to family support services consent to receiving support. The Department of Child Safety provided us with some research that indicated these consent rates are consistent with international experience. Nevertheless, there remains an opportunity for the Department of Child Safety to consider how it can work with providers of family support services to improve consent rates, particularly for those providers well below the average rate.
Of the 67,454 referrals between 2016–17 and 2018–19, family support services required consent from 52,503 families to provide support.
Of these, 49 per cent consented, but the percentage of families that consented to receive support decreased from 52 per cent in 2016–17 to 45 per cent in 2018–19.
Figure 1B shows the percentage of families that consented to receiving support for each family support service between 2016–17 and 2018–19.
Consent rates between family support service providers vary due to the differing roles they play and, for this reason, are not a valid comparison of relative performance. Family and Child Connect services provide advice to families and connect them to the right type of service, including Aboriginal and Torres Strait Islander Family Wellbeing services or Intensive Family Support services.
It is likely that Family and Child Connect services will have obtained consent before referring families to the relevant family support service. Therefore, we would expect Aboriginal and Torres Strait Islander Family Wellbeing services and Intensive Family Support services would have higher consent rates than Family and Child Connect services.
Consent rates varied significantly across regions. For example, the consent rate for Family and Child Connect services in Hervey Bay was 30 per cent, compared with 52 per cent for the Sunshine Coast (for cases referred by the Department of Child Safety between 2016–17 and 2018–19). A variety of factors may influence consent rates across regions. These include social and demographic factors, the funding and resourcing of family support service providers, the techniques they use, and the time they take to engage families.
The Department of Child Safety requires family support services to notify it if a family that it refers does not consent to receiving support. This enables the Department of Child Safety to consider this information and make an informed decision if it receives an additional child harm report. We found that family support services have not advised the Department of Child Safety of all cases as required. Between 1 July 2016 and 30 June 2019, 89 per cent (14,792) of cases where families did not consent were reported to the Department of Child Safety. This reporting needs to improve as this information is valuable for assessing future reports of harm.
Minimum requirements to engage families
The Department of Child Safety guidelines require Family and Child Connect services to attempt to contact a family at least four times over a six-week period to obtain consent before closing a case. They must attempt to contact each family by sending two letters, phoning, and making at least one visit to the family's home.
We found that some Family and Child Connect services did not comply with the minimum standards for engaging with families. Since July 2016, Family and Child Connect services closed cases for 6,792 families because they could not be located. This represents 20 per cent of all cases closed over this period. Of these:
- 1,874 cases did not have the minimum of four attempts across three mediums
- 659 cases had no correspondence recorded
- 546 cases had no home visit recorded
- 192 cases had no phone call recorded
- 38 cases had no contact recorded.
The number of cases where Family and Child Connect services did not meet the minimum attempts of engagement is likely to be higher. We excluded 3,878 cases because we could not be certain that contact had not occurred with the family due to data quality issues.
Some Family and Child Connect service providers are trialling different ways of engaging with families. In Mackay, one provider is now trialling SMS and email in addition to the standard methods. It is too early to confirm whether the trial has improved consent rates, but this demonstrates the initiative of some non-government organisations to improve engagement with families.
The Department of Child Safety does not require Aboriginal and Torres Strait Islander Family Wellbeing services or Intensive Family Support services to make a minimum number of attempts to contact a family before they close a case. We found they had closed 179 cases despite only making two or fewer attempts to contact families.
Establishing minimum expectations based on a better practice approach (for example a minimum number of attempts to contact a family) for all family support service providers may help to improve consent rates. In doing this, the department should take into consideration the need to be flexible to meet different circumstances. In some cases, family support service providers would not have the capacity to deliver services if consent rates were higher (as might occur if minimum standards were set). The Department of Child Safety advised that, for this reason, it does not expect providers to devote the same effort to obtain consent in all cases.
Time taken to engage families
The time taken by family support services to contact families could be contributing to families not consenting to receive support. When family support services are slow to engage with families, there is a higher likelihood that families will not consent.
Figure 1C shows the time taken by family support services to attempt to contact families from the date they received the referral between 2016–17 and 2018–19.
|
Provider |
Median days |
Average days |
|---|---|---|
|
Family and Child Connect services |
3 |
6 |
|
Intensive Family Support services |
7 |
12 |
|
Aboriginal and Torres Strait Islander Family Wellbeing services |
12 |
27 |
Notes: Family and Child Connect services connect families to the right support services. Intensive Family Support services and Aboriginal and Torres Strait Islander Family Wellbeing services provide specialist support to families with multiple and complex needs.
Queensland Audit Office using ARC data provided by the Department of Child Safety.
Between 2016–17 and 2018–19, 39 per cent of the families contacted within the first week consented to receiving support. In contrast, where family support services took two weeks or longer to contact the family, the consent rate dropped to 34 per cent.
Some family support service providers reported high caseloads and said they were struggling to keep up with demand. High caseloads may impact the time they take to engage with families. We could not assess their caseloads because they do not record this information in their ARC database.
Subsequent reports as an indicator of effectiveness
The Department of Child Safety assesses the outcomes for families that receive support, but it does not consider the outcomes for those families that refuse support. We tried to assess whether families that received support from family support services had fewer subsequent reports of child harm compared with those families that did not receive support. While not definitive, this can provide an indication of the effectiveness of family support services.
We could not validate this analysis because of the unreliability of the ARC data. The Commission and Department of Child Safety should further investigate the data quality and better assess the outcomes for vulnerable families referred to family support services.
A more detailed investigation may help determine the cause of the subsequent harm reports and whether there are opportunities to improve the support families receive.
Data quality
In June 2015, the Department of Child Safety implemented the ARC database. It enables family support service providers to record information about vulnerable families, such as their contact details, their circumstances, and what support they require. The system has provided a secure platform to record details about families requiring support.
There are a range of data quality issues with the ARC database. We found family support service providers are not accurately recording all children involved in cases, whether they obtained consent, or the activities they performed to engage a family.
Between 1 July 2016 and 30 June 2019, 16 per cent (12,546) of the families referred to family support services had no record of a child in the ARC database. This information is critical, particularly if the behaviour within that family escalates or the Department of Child Safety receives another report about the child's safety. This percentage was higher for some services, such as Aboriginal and Torres Strait Islander Family Wellbeing services, which had no children recorded in 30 per cent of cases over the same period.
The Department of Child Safety does not have line of sight to all children it refers to family support services. It cannot gain assurance that family support services are supporting the families it refers. This creates a risk that a family may be overlooked. Between 2016–17 and 2018–19, the Department of Child Safety recorded in its Integrated Client Management System (ICMS) that it referred 53,800 children to Family and Child Connect services and Intensive Family Support services where a report did not meet the threshold for investigation. We identified that these children related to 28,717 cases. In contrast, family support services recorded in ARC that the Department of Child Safety referred 27,046 cases to Family and Child Connect services and Intensive Family Support services. The systems do not provide a means to easily reconcile between the two databases. In addition, the Department of Child Safety has no way of reconciling referrals it makes to Aboriginal and Torres Straight Family and Wellbeing Services.
In July 2019, the Department of Child Safety conducted an internal review into the accuracy of ARC data. It identified inconsistencies in how family support services record data. It also found important information was missing from cases, such as the child's date of birth. As a result of the review, the Department of Child Safety has delivered training to family support service providers to improve the accuracy of data captured in ARC. The Department of Child Safety advises us that it is undertaking a range of actions to improve data quality, including providing additional training and support to family support service providers, and monitoring and reporting data quality.
Improving the quality of data captured in the ARC database will enable the Department of Child Safety and the Queensland Family and Child Commission to more effectively assess the impact of family support services and the outcomes achieved for vulnerable children.
2. Protecting children from harm
Introduction
When alleged harm or risk of harm is reported, child protection staff, police, educators, and health professionals must work together for the safety and wellbeing of the child. Their timely exchange of accurate and reliable information is important to avoid delays and ensure their response is effective.
The Department of Child Safety, Youth and Women (Department of Child Safety) investigates allegations that a child has been significantly harmed, is suffering significant harm, or is at risk of being significantly harmed and does not have a parent able and willing to protect them. In some cases, it is necessary for the Department of Child Safety to remove a child from their home and place them with extended family, with foster carers, or in residential care.
In this chapter we assess whether entities:
- support the appropriate reporting of children at risk
- respond efficiently and effectively to reports of harm
- place children into out-of-home care based on their needs.
Reporting allegations of harm or risk of harm
Reporting behaviour
Mandatory reporters are making a high number of reports to the child protection system that do not meet the threshold for investigation.
Between 2013–14 and 2018–19, the Department of Child Safety received 687,052 child harm reports. Approximately 80 per cent (547,261) of these reports did not meet the threshold for investigation. This remained consistently high over the six-year period.
In July 2019, the Attorney-General announced proposed reforms to legislation that will create new offences for failing to report institutional child sexual abuse. The legislation is expected to take effect this year. It is possible this legislation may increase reporting and place greater pressure on the Department of Child Safety intake services.
The Queensland Child Protection Commission of Inquiry (Carmody Inquiry) identified entities' risk-averse behaviour as the primary driver for overreporting. Entities are reluctant to carry the risk of incorrectly referring a report about a child's safety to family support services and, as such, report all concerns to the Department of Child Safety.
The Carmody Inquiry recommended two reporting pathways to enable reporters to refer directly to family support services any concerns about a child's safety that do not meet the threshold for an investigation, and to report concerns of significant harm to the Department of Child Safety. The intent of the reform was to divert child safety concerns away from the child protection system and toward the family support system. The reform has not achieved its intended outcome. Entities remain cautious about the ramifications of failing to report.
Queensland's existing family support and child protection system relies on mandatory reporters to understand their reporting obligations. It requires mandatory reporters to make an informed decision based, at times, on limited information. Mandatory reporters may report harm based on valid concerns about a child’s safety, which upon expert assessment by the Department of Child Safety may not require an investigation. Nevertheless, these reports may help assess cumulative risk of harm to a child.
For some mandatory reporters, perceived risk is a key driver of their reporting behaviour. In April 2020 we received legal advice from the Department of Child Safety confirming that mandatory reporters do not commit an offence for failing to comply with the mandatory reporting provisions under the Child Protection Act 1999. However, some mandatory reporters are legally responsible for reporting harm under other pieces of legislation. For example, a teacher can be charged for failing to report sexual abuse to the Queensland Police Service under the Education (General Provisions) Act 2006. Given the misconception held by some mandatory reporters, additional education about the legislative responsibilities of mandatory reporters and the ramifications for failing to report would be of value.
The Department of Education was the highest contributor of reports that did not meet the threshold when compared to other mandatory reporters. Only one in every five reports it made over the six-year period met the threshold for significant harm. In 2017–18, the number of reports it made that did not meet the threshold increased by 59 per cent following a campaign by the Queensland Teachers Union in November 2017 to encourage reporting. The campaign, Report everything; report often; report in writing, was the result of a teacher investigated (although not prosecuted) for failing to report sexual abuse to the Queensland Police Service under the Education (General Provisions) Act 2006.
Teachers report child safety concerns to their respective principals using the Department of Education's One School system. The system enables teachers to effectively report child harm but lacks the capability to refer to family support services any reports that do not meet the threshold for investigation. As such, the Department of Education requires its staff to re-enter their concerns about a child's safety into another system, duplicating effort.
School principals assess whether a teacher's concerns about a child meet the threshold of significant harm and whether they need to report it to the Department of Child Safety. The Department of Education has seven Student Protection Principal Advisors who assist principals with their reporting obligations. The number of principals across the state limits their influence. As at May 2020, there was one Student Protection Principal Advisor to every 156 principals.
The Department of Education provides regular training to teachers and principals about their reporting obligations. It could improve the training it provides teachers and principals to better inform them of the reporting pathways and the threshold for investigation. The existing training understandably focuses on the mandatory reporting obligations of teachers and principals. The training could be enhanced by providing them with information and guidance about appropriate circumstances for referring families to family support services and further encouraging them to utilise the existing online Queensland Child Protection Guide, the Department of Education’s Student Protection Principal Advisors and the Department of Child Safety’s child safety officers to help inform reporting decisions.
Some mandatory reporters take a more proactive approach to managing reports of alleged harm or risk of harm before referring them to the Department of Child Safety. The Queensland Police Service relies on its 35 Child Protection and Investigation Units and its SCAN (suspected child abuse and neglect) representatives, who are responsible for child protection responses, including criminal investigations. These units screen reports of alleged harm or risk of harm made by police officers to assess the action required, including whether to report it to the Department of Child Safety, refer it to family support services, or take no further action. In 2018–19, 38 per cent of its reports met the threshold, compared with only 17 per cent reported by the Department of Education. The Queensland Police Service has an effective referral system that enables police officers to easily refer to family support services any concerns about a child's safety that do not meet the threshold.
Screening reports
Intake services
Timely and effective screening of child harm reports is critical to determine whether a child may be in need of protection and how quickly the Department of Child Safety needs to investigate. Its eight intake services and one after-hours service screen the reports and assess whether they meet the threshold for investigation. To make that assessment, they can gather information from a range of stakeholders, such as school attendance records and medical history, when further information is needed to assist in deciding the appropriate response. Staff use a structured tool that guides them in their decision-making process. They give priority to reports that indicate a child is in immediate danger. They can also refer to the department's child safety practice manual for additional guidance.
The Department of Child Safety's existing intake model results in inefficiencies. Across the eight intake services there are inconsistent practices in triaging reports, allocating work, recording child harm reports, and providing feedback to mandatory reporters.
Some practices result in delays to screening and investigating child harm reports. In some regions, intake services do not allocate child harm reports to intake staff if their workloads are high. Instead, they wait until staff have additional capacity to work through the unallocated reports.
We also found that the after-hours service centre has limited capacity to respond to child harm reports. The Department of Child Safety only has one after-hours service centre, which is located in Brisbane and services all of Queensland.
Some intake staff manually record a child harm report in a Word document, and then re-enter it into the Integrated Client Management System (ICMS). Other regions directly enter the report into ICMS. The Department of Child Safety intends to roll out a new program by the end of December 2020 to improve the quality and consistency of its intake services’ administrative processes and practices.
The feedback that intake services provide to mandatory reporters is inconsistent and, at times, lacks the detail required to change reporter behaviour. Mandatory reporters would benefit from consistent feedback about the outcome of a report and the rationale for the outcome.
The existing intake model puts the onus on the Department of Child Safety and does not apply a system-wide approach. Establishing a multi-disciplinary intake process that integrates information from all relevant agencies is likely to improve interagency coordination and the timely and effective screening of reports. The Department of Child Safety should retain accountability for the final decision regarding the most appropriate action to take for each child harm report. It is currently considering changes to its intake model to improve consistency and the more efficient triage of child harm reports.
Of the 687,052 reports screened by intake services between 2013–14 and 2018–19:
- intake services referred 20 per cent (139,791) of cases to child safety officers for investigation because they met the threshold for investigation
- intake services referred 14 per cent (93,311) of cases to family support services because they did not meet the threshold for investigation and they decided the family would benefit from additional support
- intake services closed 66 per cent (453,950) of cases and took no further action because they were not able to form a reasonable suspicion that the child needed protection and decided the family would not benefit from additional support.
In some cases, where intake services decided to close a case and not refer it to family support services, the Department of Child Safety received an additional child harm report about the child within 12 months.
Between 2016–17 and 2018–19, intake services chose not to refer 204,273 child harm reports that did not meet the threshold for investigation. We found that, for eight per cent (16,332) of these, the Department of Child Safety received a subsequent report within 12 months that met the threshold for investigation. Of these, 38 per cent (6,222) of the reports resulted in an investigation that substantiated the child had experienced significant harm or was at unacceptable risk of significant harm.
The 6,222 reports relate to 3,354 individual children. We cannot confirm whether the decision to not refer the original child harm report to family support services would have prevented the subsequent child harm report. In some instances, family circumstances change after intake services make their initial assessment. Nevertheless, there would be value in the Department of Child Safety reviewing some of the original decisions to not refer these cases to determine whether it needs to improve its decision-making process.
Time taken to screen child harm reports that did not meet the threshold for investigation
The Department of Child Safety has improved its timeliness in screening and referring child harm reports that do not meet the threshold for investigation to family support services, from a median of 10 days in 2016–17 to seven days in 2018–19. In some cases, intake services take a lot longer to refer child harm reports.
Despite these improvements, more than 14 per cent (4,396) of child harm reports took longer than one month to refer to family support services between 2016–17 and 2018–19. These delays inhibit family support services engaging with families early and can impact on a family's willingness to consent.
The Department of Child Safety does not have a target for how long it should take to refer child harm reports to family support services. A target may help ensure timelier referral of all child harm reports and earlier support to families. In developing a target, the Department of Child Safety would need to ensure it continues to prioritise child harm reports that meet the threshold for investigation.
Across regions, there was a significant variation in the time taken to refer child harm reports to family support services, ranging from a median of six days for the Moreton region to 13 days for the south east region.
Understandably, the Department of Child Safety intake staff defer screening and referring child harm reports to prioritise those reports that meet the threshold for investigation. The Department of Child Safety could improve its timeliness and reduce staff effort in referring child harm reports to family support services by automating the transfer of these reports between ICMS and the family support services' Advice, Referrals and Case Management (ARC) database.
Time taken to screen child harm reports that met the threshold for investigation
The Department of Child Safety requires its intake services to screen reports that meet the threshold for investigation within 48 hours of receiving the initial information. Intake services are not meeting this performance target. Of the 139,791 reports that met the threshold for investigation between 2013–14 and 2018–19, intake services screened 63.3 per cent (88,421) within 48 hours.
When a report meets the threshold for investigation, intake services staff use a structured decision-making response priority tool to set an initial time frame for how quickly child safety officers need to commence the investigation—either 24 hours, five days, or 10 days. The risks considered include the severity of the child's injuries, immediate safety concerns, age, and history.
Figure 2A shows that, between 2013–14 and 2018–19, intake services were quick to prioritise reports that indicate a child is in immediate danger and requires a 24-hour response, but not so quick for the other priority categories.
|
Response priority |
Median |
Average |
|---|---|---|
|
24-hour priority |
2 hours and 45 minutes |
25 hours and 29 minutes |
|
5-day priority |
23 hours and 36 minutes |
3 days, 22 hours, and 6 minutes |
|
10-day priority |
46 hours and 24 minutes |
5 days, 20 hours, and 34 minutes |
Notes: The median and average time taken by intake services to screen a report have been calculated from the time the report was received by the intake services to the time it took intake staff to record a child harm report for investigation. It does not include the time taken by the team leader to approve the report for investigation.
Queensland Audit Office using ICMS data provided by the Department of Child Safety.
The Department of Child Safety screened 91.8 per cent of all reports that required a 24-hour response within the required 48 hours. Over the six-year period, the time taken to screen reports that required a 24-hour response remained steady.
The time taken to screen reports that required a five- or 10-day response was much higher. Intake services screened within 48 hours 66 per cent of all reports that required a five-day response. They screened within 48 hours 51 per cent of all reports that required a 10-day response. Although these reports are less urgent, timely investigation is critical to ensure a child is safe.
Figure 2B shows a significant variation in the time taken by intake services to screen reports requiring a 10-day response.
Queensland Audit Office using ICMS data provided by the Department of Child Safety.
In 2018–19, the median time the south west regional intake service took to screen child harm reports requiring a 10-day response was 304 per cent higher than in 2013–14—from one day and five hours in 2013–14 to four days and 20 hours in 2018–19. Similarly, the median time the northern regional intake service took increased by 226 per cent—from one day in 2013–14 to three days and seven hours in 2018–19. Both regions also had an increase in the time taken to screen child harm reports that required a five-day response.
In contrast, central and Moreton region were screening child harm reports requiring a 10-day response quicker in 2018–19 than in 2013–14.
Various factors can influence the difference in the time taken between intake services to screen reports, including natural disasters, behaviour of mandatory reporters, differences in social demographics, resourcing levels, and inconsistent screening practices.
Sharing information to screen child harm reports
The timely sharing of information between entities is critical to determine the most appropriate response and respond to the child’s safety and support needs. We looked at one aspect of information sharing during the screening process—when intake services seek additional information about a child from entities, such as their school attendance records. Delays by entities to share information may be due to the volume of requests (including duplicate requests), the breadth of information requested, the clarity of the request, and the rationale given by the Department of Child Safety for why they require the information.
The Department of Child Safety regional intake service staff across the state expressed frustration at delays in obtaining information from external entities (such as police, education, and health) necessary for them to assess reports and determine the most appropriate response.
Contrary to what we were told, our data analysis showed that police officers, teachers, and hospital professionals were quick to provide information to intake services for reports that required a 24-hour response and reasonably timely for child harm reports requiring a five- and 10-day response.
The timely sharing of information has remained relatively consistent year-on-year between 2014–15 and 2018–19. There is, however, room to further improve the timeliness of information sharing.
Figure 2C displays the average time taken by stakeholders to share information with intake services from the time they received the request between 2014–15 and 2018–19.
The south west regional intake service was the only intake service to experience significant delays obtaining information from stakeholders for child harm reports that did not meet the threshold for investigation. Between 2014–15 and 2018–19, it took police officers in the south west region on average six days and four hours to respond to 4,037 information requests from the intake service. Although these information requests were for reports that did not meet the threshold for investigation, the delays inhibited timely referral of families requiring support.
The Queensland Police Service, in collaboration with the Department of Child Safety, has implemented a new system that enables intake service staff to access police records for a person's criminal and domestic violence history. This will help intake service staff make more timely decisions during the screening process.
Responding to allegations of harm or risk of harm
Investigating child harm reports
The Department of Child Safety has 59 child safety service centres across the state responsible for investigating allegations that a child has been significantly harmed, is suffering significant harm, or is at risk of being significantly harmed and does not have a parent able and willing to protect them. Child safety officers gather information from various sources to assess whether a child is in need of protection.
Between 2013–14 and 2018–19, the Department of Child Safety investigated 135,791 child harm reports. In 30.5 per cent (41,404) of these investigations, child safety officers substantiated that the child had suffered significant harm or was at unacceptable risk of significant harm.
For the remaining 94,387 children, child safety officers could not substantiate harm or risk of harm, could not sight the child, or the investigation was ongoing. For some of these investigations, a child safety officer may have sought consent from the family to refer them to family support services.
Timely commencement of investigations
Prior to September 2019, the Department of Child Safety defined the commencement of an investigation as the date its child safety officers sighted a child. For reports that required a 24-hour response, it measured the number of calendar days from when the intake centre first received the child harm report to the time the child safety officer sighted the child. For investigations with a five- or 10-day response priority, it measured the number of business days from when the intake service first received the child harm report to the time the child safety officer sighted the child.
It has since changed these requirements and now only requires child safety officers to sight a child within a prescribed time frame for reports requiring a 24-hour response. The Department of Child Safety changed its target to better align with the reforms from the Carmody Inquiry and available resources.
For five- and 10-day priority reports, the Department of Child Safety now measures the time taken by child safety officers to start gathering information for the case. Its child safety officers must still sight a child, but there is no longer a requirement to sight a child within a specified time frame. We discuss the Department of Child Safety’s new practice approach for measuring and reporting the timely commencement of its investigations in chapter three.
We have assessed the performance of child safety service centres (service centres) against the performance metrics the Department of Child Safety used between 2013–14 and 2018–19.
Service centres are quick to commence child harm reports that require a 24-hour response. Between 2013–14 and 2018–19, the median time child safety officers took to sight a child was 19 hours and 12 minutes (from the time the intake service received the child harm report). Service centres have maintained a timely response for these most urgent cases over the six-year period. Their timely response to these reports was crucial given they assessed these children as being in immediate danger.
The timely commencement of all investigations is essential, including those child harm reports that require a five- and 10-day response. The Department of Child Safety is not timely in commencing an investigation for reports that require a five- and 10-day response.
The median time service centres took to sight a child for reports that required a five-day response increased from 15 business days in 2013–14 to 21 business days in 2018–19. Similarly, the median time service centres took to sight a child for child harm reports that required a 10-day response increased from 22 business days in 2013–14 to 32 business days in 2018–19. The average, however, is much higher, indicating that some service centres are not sighting children for more than a month after they receive the initial report of harm.
Figure 2D shows how long the Department of Child Safety took to sight a child for reports that required a five- and 10-day response between 2013–14 and 2018–19.
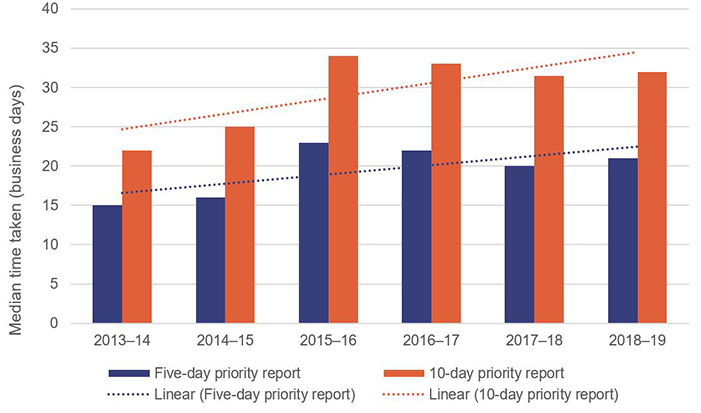
Notes: We assessed the time taken by a child safety officer to sight a child from when the intake service first received the child harm report to the time the child safety officer sighted the child. We calculated the time taken to sight a child based on business days.
Queensland Audit Office using ICMS data provided by the Department of Child Safety.
The Department of Child Safety's regions vary significantly in how long they take to sight a child for reports that require a five- and 10-day response.
The median time taken by the south east region to sight a child for reports that required a five-day response increased by 76 per cent—from 21 business days in 2013–14 to 37 business days in 2018–19. It also had the greatest delay for sighting a child for reports that required a 10-day response. This is despite its total number of reports requiring investigation decreasing from 4,005 in 2013–14 to 3,445 in 2018–19.
In contrast, the median time it took the Moreton region to sight a child for reports that required a five-day response was 17 business days over the six-year period. It also reduced the median time it took to sight a child for reports that required a 10-day response over the six-year period. This is despite a five per cent increase in the number of five- and 10-day priority reports that required investigating. Appendix F captures the time regions took to investigate 24-hour, five-day, and 10-day priority reports.
The cause of delays to sight a child is likely to be varied. In some cases, the complexity of the case and/or the geographical location of the child will influence the time taken to investigate a report of harm. High caseload per child safety officer is another possible reason for delays to sight a child. Regions with the highest staff turnover and the highest transfer of staff between regions (central, northern, and south east regions) also had the longest delays to sight a child. In contrast, Moreton region had the lowest staff turnover and shortest times to commence an investigation.
A child safety officer's role is both challenging and demanding. In 2018–19, one in every four child safety officers either left the Department of Child Safety or transferred to another region.
The Department of Child Safety staff from four of the five regions we visited reported to us a lack of training and support to child safety officers to effectively perform their role. This included concerns raised by child safety officers and management across regions about both induction and ongoing training.
Over the past 10 years, the amount of formal classroom-style training provided to child safety officers at induction has reduced from eight weeks to two. The Department of Child Safety changed its approach to induction training for new child safety officers to a combination of face-to-face training, online training, on-the-job coaching, and mentoring, to better develop the capability of its staff. A blended approach is likely to improve the capability of its child safety officers, but the Department of Child Safety also needs to ensure the training provided is sufficient to meet their learning needs.
Staff and managers from four of the five regions we visited reported that child safety officers carried high caseloads and, at times, did not receive adequate support and mentoring. We also heard from team leaders who said they were unable to provide sufficient coaching due to workload. Improving the support and training provided to child safety officers is likely to help reduce staff movement.
The Department of Child Safety is currently looking at how it can provide better support to its child safety officers. It has developed a workload management policy and manual to better manage workloads and intends to develop an induction toolkit to support new child safety officers by late 2020. In collaboration with the Queensland Family and Child Commission, it is also reviewing its investigation and assessment strategy to identify opportunities to improve timely commencement and streamline the process.
In some cases, the Department of Child Safety and the Queensland Police Service may jointly investigate a child to ensure they are safe. The agencies report that these joint investigations are working well, although there remains an opportunity to improve the timely sharing of information and decision making. The Queensland Police Service did report that, in some instances, child safety officers from the Department of Child Safety had requested police to sight a child and report back to them on the child’s welfare. The Queensland Police Service does not support this practice given its officers do not have the necessary knowledge and experience to effectively assess a child’s protective needs.
Completing investigations
Up until 1 September 2019, the Department of Child Safety required child safety officers to complete an investigation within 60 calendar days from the date the service centre received the report. Between 2013–14 and 2018–19, the Department of Child Safety completed 46.3 per cent of its investigations within 60 days. The percentage of investigations completed within 60 calendar days has decreased from 60.1 per cent in 2013–14 to 41 per cent in 2018–19.
From July 2014, the Department of Child Safety implemented a new practice approach in response to the reforms from the Carmody Inquiry. Its new approach involves staff spending more time working intensively with families during the investigation phase to de-escalate family risks and increase safety for children. It hoped this would result in fewer children requiring protection. The Queensland Police Service raised concerns with us over this new practice approach, highlighting that at times there may be a conflict between the interests of the child and the interests of the adult caring for the child. The Department of Child Safety’s child safety practice manual clearly states that the best interests of the child are to be at the centre of all decision making.
The number of investigations where harm was substantiated and the child was in need of protection has decreased from 4,494 in 2017–18 to 3,842 in 2018–19. Various factors could have contributed to this decrease, such as the reduction in the number of investigations over this period. We were unable to determine the extent to which the change to the Department of Child Safety's investigation approach may have contributed to this decrease. The number of children in care has increased as children are staying in care longer.
The median time the Department of Child Safety took to complete investigations for 24-hour, five-day, and 10-day priority reports increased over the six-year period.
Figure 2E shows the median time the Department of Child Safety took to complete investigations between 2013–14 and 2018–19.
Notes: The median time taken to complete investigations has been calculated from the time the intake service received the child harm report to the time it took for the child safety officer to complete the investigation and assess whether the child experienced significant harm or was at risk of significant harm and whether the child was in need of protection. We calculated the time taken to complete an investigation based on calendar days. This is consistent with how the Department of Child Safety measured the time taken to complete an investigation between 2013–14 and 2018–19.
Queensland Audit Office using ICMS data provided by the Department of Child Safety.
Removing children from harm
Difficulty finding suitable placements for children who require out-of-home care is putting pressure on the child protection system and creating instability for children.
The Department of Child Safety places a child into out-of-home care when it assesses that they are unable to remain safely in the care of their family at home. Out-of-home care includes:
- kinship care—placing a child in the home of a family member who is approved as a kinship carer and who receives payments for caring for the child
- foster care—placing a child in the home of a carer who is not kin and who receives payments for caring for the child
- residential care—placing a child in a residential facility, with paid staff who care for the child.
When placing children into care, the Department of Child Safety must comply with the National Standards for out of home care and standards under s. 122 of the Child Protection Act 1999. These standards include:
- placing children into care that best matches their needs and ensures their ongoing safety
- ensuring children are provided with stability and security during their time of care.
Placing a child into a care arrangement that does not match their needs or that cannot provide the support they require is unlikely to achieve stability for the child and can have significant adverse effects on the child. Government and academic studies nationally and internationally have found that continued instability is associated with poor educational, employment, social, behavioural, and emotional outcomes for children.
A shortage of foster carers is making it increasingly difficult for the Department of Child Safety to find appropriate out-of-home care for children. The complexity of children's behaviour, the cost of caring, and the increasing number of families with two working parents are some of the reasons why there are fewer foster carers. The existing requirements placed on foster carers and next of kin carers can also be arduous. In some instances, the Department of Child Safety requires home-based carers to seek permission before making basic life decisions if they are not the long-term or permanent guardian for the child. For example, it requires some home-based carers to seek permission before taking a child on a family holiday or going to the hairdresser. These requirements impact on the willingness of people to become foster carers and the ability for children to integrate into a stable family environment.
The number of children in out-of-home care increased by 19 per cent from 8,631 in 2013–14 to 10,248 in 2018–19. In contrast, the number of foster carers has only increased by 10.6 per cent from 4,833 in 2013–14 to 5,345 in 2018–19. In addition, the number of children staying in care longer is increasing, reducing the availability of carers.
Child safety officers and managers from two of the five regions we visited reported to us instances of staff needing to work late and keep a child at the service centre until they could find a place for the child to stay. The Department of Child Safety service centres do not have appropriate facilities to support and care for children while staff try to find a suitable placement. None complained about doing this, but they raised concerns over the shortage of foster carers and the quality of care provided by residential care facilities.
The lack of placement options also affects other entities, like the Queensland Police Service. In the last 12 months alone, we identified five examples where young adolescents slept overnight in police stations due to a lack of placement options. Their carers either refused to collect them or allow them to return to their care facilities because of their complex behavioural needs. In several of these cases, the Queensland Police Service contacted the Department of Child Safety to find an alternative placement, but was unsuccessful, and the child remained in the care of police overnight.
It is likely that difficulties in matching children to the most appropriate care based on their needs and circumstances is contributing to a higher number of placement changes.
Figure 2F shows that, of the 10,468 children placed into care between 2013–14 and 2018–19, only 26 per cent (2,762) of children had one placement. Almost a quarter of the children placed into care by the Department of Child Safety had between six and 30 placements over the six-year period.
|
Number of placements |
Number of children |
Percentage |
|---|---|---|
|
1 placement |
2,762 |
26% |
|
2–5 placements |
5,205 |
50% |
|
6–10 placements |
1,841 |
18% |
|
11–20 placements |
626 |
6% |
|
21–30 placements |
34 |
0% |
|
Total |
10,468 |
100% |
Notes: Some children may have already been in care prior to 2013–14. Percentages have been rounded to whole numbers.
Queensland Audit Office using ICMS data provided by the Department of Child Safety.
In November 2018, the Department of Child Safety started a care-enhancement project focused on providing better stability and outcomes for children in care. The project's initiatives include increasing the number of children placed with kin and increasing the number of foster carers. It has engaged five non-government organisations to identify and successfully place children with kin.
Residential care
Across Australia, it is recognised that family-based care (kinship care and foster care) is the preferred model of care for children requiring protection. In Queensland, residential care is for children who have extreme or specific needs and who are not suited to family-based care. The Department of Child Safety is finding it increasingly difficult to find suitable placements for children, outside of residential care. In Queensland, the number of children in residential care has increased by 45 per cent, from 656 in 2013–14 to 951 in 2018–19.
Across the state, child safety officers reported concerns about the quality of care provided by residential care facilities. Staff from four of the five regions, and staff from other government and non-government agencies, raised concerns over the care provided by residential facilities. We heard that in some instances:
- children were placed into residential care due to the limited capacity of other placement options, rather than to match their individual needs
- children were placed into environments that were unsuitable and sometimes worse than where they had come from.
Residential care facilities are staffed by shift workers who rotate every 12 hours. As such, they often lack the steadiness children require to feel safe and secure. Many of the shift workers do not have the appropriate qualifications, training, or experience to effectively support the children placed in their care. The Department of Child Safety has introduced minimum qualification standards for residential care staff effective from 1 January 2019. These standards are intended to help improve the care that is provided to children in residential care facilities.
The Queensland Government states on its caring for children website that residential care is primarily for young people aged 12 to 17 years with complex and extreme support needs. Despite this, it is placing a high percentage of children under 12 years of age into residential care facilities. Between 2013–14 and 2018–19, almost one-third of children placed in residential facilities were below the age of 12. The Department of Child Safety needs to improve the quality and availability of out-of-home care options available to children requiring care.
Indigenous children in care
The over-representation of Indigenous children in the child protection system is a long-standing national issue. In June 2013, the Carmody Inquiry stated that Indigenous children are nine times more likely to be placed in out-of-home care than non-Indigenous children.
In 2018–19, 43 per cent of all children in care were Indigenous. In contrast, Indigenous children made up only eight per cent of children in Queensland.
The Aboriginal and Torres Strait Islander Child Placement Principles sets out the preferred placement options for Aboriginal and Torres Strait Islander children. Its preferred option is to place Aboriginal and Torres Strait Islander children with kin or the child's Indigenous community. Its least preferred option is to place them with non-Indigenous carers. Between 2013–14 and 2018–19, the Department of Child Safety placed 44 per cent of Indigenous children into care with non-Indigenous carers. This remained consistent over the six-year period.
Much work is occurring to reduce the number of Indigenous children in the child protection system. The Queensland government's Our Way: A generational strategy for Aboriginal and Torres Strait Islander children and families 2017–2037 (Our Way strategy) provides a blueprint for how the government aims to improve outcomes for Indigenous children. It is supported by Changing Tracks: An action plan for Aboriginal and Torres Strait Islander children and families 2017–2019. Recent actions have included:
- establishing the Queensland First Children and Families Board in November 2018 to oversee implementation of the Our Way strategy
- establishing 33 non-government organisations to deliver Aboriginal and Torres Strait Islander Family Wellbeing services (established between December 2016 and April 2018)
- amending the Child Protection Reform Amendment Act 2017 in October 2018 to embed the Aboriginal and Torres Strait Islander Child Placement Principles.
In December 2018, the Queensland First Children and Families Board reported on the progress achieved. Since January 2018, Queensland has stabilised the proportion of children in care who are Aboriginal and Torres Strait Islander, despite the number increasing nationally.
3. Managing the system
Introduction
Caring for children and keeping them safe is a responsibility shared across government, non-government organisations, and the broader community. Queensland's family support and child protection system (the system) requires all entities to work together effectively and efficiently to ensure children are safe, healthy, and supported.
Appropriate governance and system oversight are necessary to manage the system and make sure there is effective and efficient coordination across entities. Monitoring and reporting performance at both an entity and system level enables entities to identify risks and gaps in services and drive improvement.
As a result of the Queensland Child Protection Commission of Inquiry (Carmody Inquiry), the Queensland Government established governance structures to oversee system reform. This included the Interdepartmental Committee and nine regional committees. Additional committees and groups form part of the broader governance.
The Interdepartmental Committee is responsible for leading government policy on child protection, youth justice, and domestic and family violence reforms. The Deputy Director-General of the Department of the Premier and Cabinet and the Director-General of the Department of Child Safety, Youth and Women (Department of Child Safety) chair the committee. Its membership comprises 14 public sector entities.
Across Queensland there are 13 Regional Child, Youth and Family Committees responsible for implementing reform from the Carmody Inquiry. Committee membership includes representatives from government and non-government organisations.
Under the Family and Child Commission Act 2014, the Queensland Family and Child Commission (the Commission) performs a range of functions, including:
- oversight of the system
- strengthening capacity and capability
- educating families, communities, and professionals about services available to support Queensland families.
The Commission performs its oversight function by evaluating and reporting on the performance of the system. The Department of Child Safety also monitors and reports on service delivery across the system.
This chapter assesses the adequacy of the system's governance and oversight arrangements.
It also examines whether entities monitor and report performance at an entity and system level and use this information to drive improvement across the system.
Governance and oversight
Queensland's family support and child protection system has appropriate governance vehicles and oversight to ensure the system is performing effectively. However, the role and purpose of these committees needs to be better defined to strengthen system governance and oversight. Enhancing communication between the committees is also likely to improve the effectiveness of these governance arrangements and result in better outcomes for the system.
Committees
The Interdepartmental Committee and the 13 Regional Child, Youth and Family Committees provide an avenue for entities to share information, discuss key issues, and drive improvements across the system. Enhancing the communication channels between the Interdepartmental Committee and regional committees is likely to improve the effectiveness of these governance arrangements and result in better outcomes for the system.
The Interdepartmental Committee's primary role has been to oversee and monitor the implementation of the reform from the Carmody Inquiry. Since its establishment, it has regularly monitored reform implementation.
There is opportunity for the Interdepartmental Committee to take a greater role in providing leadership and governance of the system. Specifically, the Interdepartmental Committee is appropriately placed to coordinate cross-agency efforts to address systemic issues, such as the number of children placed into care and the over-representation of Indigenous children in the system. The Interdepartmental Committee also needs to provide greater direction to regional committees to ensure risk is collectively managed. These initiatives would require a change to its terms of reference.
The Department of Child Safety’s Regional Child, Youth and Family Committees provide a way to share relevant child safety information between entities. While these committees enable collaboration and information sharing, we heard from several committee members that the meetings lacked direction and were no longer action oriented.
The Department of Child Safety reviewed the Regional Child, Youth and Family Committees and reported that some had a high proxy attendance. Staff from three of the five regions we visited also reported a high proxy attendance and said that some entity representatives lacked the experience and authority to support decision making. The Department of Child Safety is currently developing a draft governance framework and other tools to ensure the appropriate flow of information between the various committees.
The Department of Child Safety is responsible for leading the 13 committees. But given these committees are part of the system's overall governance structure and have a multi-agency focus, there is value in other public sector entities sharing responsibility for leading these committees.
Oversight by the Queensland Family and Child Commission
We found that the Commission is fulfilling its legislated responsibilities, including its mandate to provide oversight of the system. It is continuing to mature how it performs its oversight function.
Since its establishment, the Commission has performed a range of reviews and inquiries. These reviews have helped identify key issues and have driven change across the system. In some instances, the Commission has been directed by government to perform a review triggered by a child's death, such as the review When a child is missing: Remembering Tiahleigh – A report into Queensland's children missing from out-of-home care and A systems review of individual agency findings following the death of a child.
Some stakeholders are not informed about the role of the Commission and how it is fulfilling its role. While the Commission’s work has included reviews of the deaths of individual children the Commission has performed more sweeping reviews to identify areas for improvements across the system. The confidential nature of some of its work and its reporting requirements may be other reasons stakeholders are not informed about the Commission.
Under its enabling legislation the Commission is not required to have an oversight strategy. It advised that it developed draft oversight strategies in 2015 and 2016, using these to inform the direction of its oversight work. As these were not accessible to outside entities this may have contributed to confusion around its role and how it is fulfilling its oversight function. The Commission advised that in July 2020 it completed its Oversight Strategy 2020 – 2022, which outlines its oversight functions and identifies strategic focus areas for the next two years. It intends publishing the strategy online shortly.
In late 2018, the Commission commenced a project to identify key points of risk for vulnerable children within the system and intends to use these high-risk areas to inform the basis of its future reviews and evaluations. This has been captured in its new oversight strategy 2020–2022. The Commission intends to embed a systems thinking approach to its vulnerability project and other priorities. A systems thinking approach will examine the linkages and interactions between the key elements of the system. Finalising its vulnerability project and its oversight strategy will ensure the Commission focuses on the most pressing system issues and provide greater visibility of its proposed program of work. We note key aspects of the system that it has not reviewed include finding suitable placement for children requiring out‑of‑home care, assessing the effectiveness of family support services, and the outcomes for vulnerable children.
Queensland's integrity agencies could enhance their oversight of the family support and child protection system through greater coordination of their planned activities. The Commission could help agencies to coordinate their planning of assurance activities across the system. Separate to this, there will be the need for integrity agencies to respond to specific incidents.
The Commission is also responsible for evaluating the implementation, outcomes, and impact of the reform from the Carmody Inquiry. The Carmody Inquiry requires the Commission to complete a five- and 10-year evaluation of the reforms. In addition to these evaluations, reform stakeholders agreed the Commission would conduct a three-year evaluation to get an early indication of progress against the reform. It completed its three-year evaluation of the reform implementation in November 2018 and after government consideration was published in October 2019, one year and seven months after its due date. Some of these delays were outside its control and, as an independent statutory body, it could not submit its evaluation report directly to Cabinet. The evaluation assessed the reform implementation from 1 July 2014 to 30 June 2017.
Monitoring and reporting performance
Entities monitor and report on the performance of Queensland's family support and child protection system, but they could improve the information they report at both an entity and system level.
System reporting
We found the performance information reported on the child protection system to be adequate, but not the performance reporting of family support services.
The Department of Child Safety and the Commission report detailed information about the performance of the child protection system. The performance information reported is useful to both child safety stakeholders and the broader public. The performance data identifies risk factors in child abuse, including the increasing number of children requiring protection who have a parent using methamphetamines. It also identifies key trends, such as the number of investigations that substantiate harm and the number of children who re-enter the child protection system. This information can help inform decision-makers and identify opportunities for improvement.
The Department of Child Safety and the Commission, in collaboration with non-government organisations, can improve the information they capture and report on the performance of family support services. The current performance information is insufficient to determine the effectiveness of family support services. It focuses primarily on the output of family support providers, such as the number of enquiries they receive, and provides no indication about their effectiveness.
Entity reporting
The Department of Child Safety reports the time it takes to commence an investigation and sight a child, and the time taken to complete an investigation.
Reporting the time taken to commence an investigation
The Department of Child Safety could improve its publicly reported performance data to more clearly report the time taken to commence an investigation. It does not clearly state that the time taken to commence an investigation includes three days to screen a report of harm. Its publicly reported data gives a perception that it commences investigations more quickly than the reality.
For example, it reported that 92.5 per cent of its investigations with a 24-hour priority commenced within that time frame for the 2018–19 financial year. In reality, 92.5 per cent of its investigations took up to four days to commence and sight a child, when allowing the three days to screen child harm reports and conduct the checks necessary to determine whether the report meets the threshold for investigation.
In addition to this, its publicly reported data does not state that the time taken to commence investigating five- and 10-day priority reports is based on business days, not calendar days. It measures timeliness using business days because its child safety officers work five days a week. Although this is reasonable, without clearly stating this it leaves the performance data open to misinterpretation. Reporting the time taken to commence an investigation based on business days shows a timelier response when compared to the number of calendar days.
Figure 3A displays the median time taken to commence an investigation for reports that required a 10-day response in business days and calendar days between 2013–14 and 2018–19, from the time the intake service received the child harm report to the time the child was sighted.
Queensland Audit Office using ICMS data provided by the Department of Child Safety.
Assessing timeliness
The Department of Child Safety has recently changed its practice and associated reporting to measure the time taken to commence and complete investigations. It reported that its existing practice required change to better align with the reforms from the Carmody Inquiry and available resources. In September 2019, it changed its measure of commencing an investigation from the time taken to sight a child to the time taken to gather new information. This change better aligns its practice with other states and territories.
It is reasonable to include the time taken to gather new information when assessing timeliness to commence an investigation. But there is also value in measuring and reporting on how long it takes the Department of Child Safety to ensure the child is safe. Both metrics used together provide a complete and transparent picture of the time taken to investigate a report of harm and ensure a child is safe.
The Department of Child Safety developed guidance material for staff on its changes to commencing an investigation. It defines gathering information as seeking and receiving new information that informs the assessment about the safety of the child or the safety of the unborn child:
- from an external agency, including a government or non-government agency, service provider, or health professional, such as a general practitioner
- through email, phone or face-to-face discussion, receipt of an information request form, a SCAN (suspected child abuse and neglect) team meeting, or a locally convened panel process with relevant partners.
In isolation, these criteria do not provide adequate assurance that a child is safe. Greater clarity around this definition is necessary to ensure gathering information adequately prioritises verifying the child's safety.
The Department of Child Safety has also removed the requirement to sight a child within a specified time frame for five- and 10-day priority reports stating that its existing resources were insufficient to meet these targets. While it is appropriate to ensure practice requirements are achievable and relevant, removing them entirely may result in greater delays and increased risk to children. To help mitigate this risk, the Department of Child Safety has engaged the Commission to monitor the timeliness of its investigations. The Department of Child Safety and the Commission should closely monitor the implementation of the practice changes to ensure information verifying a child's safety is obtained as early as possible.
The Department of Child Safety has also changed its measure to assess the time taken to complete an investigation from 60 days to 100 days. The Department of Child Safety is now spending more time working intensively with families during the investigation to de-escalate the risk to the child, which has lengthened the time taken to complete an investigation. Other jurisdictions, such as Victoria, Western Australia, South Australia, Northern Territory, and Tasmania, all require their child safety officers to complete their investigations in less than 42 days from when they receive the investigation. Unlike Queensland, these jurisdictions do not have a requirement to sight all children during an investigation.
Continuous improvement
Entities have made good progress implementing recommendations from the Carmody Inquiry. As at 30 June 2019, the Department of the Premier and Cabinet reported that entities had implemented 107 of the 121 recommendations. We did not assess whether the entities implemented the 107 recommendations.
The Department of the Premier and Cabinet reports that five of the remaining 14 recommendations outstanding have been delivered but need to be formally closed. The remaining nine outstanding recommendations directed to the Department of Child Safety relate to legislative changes, reducing red tape, and reviewing the capacity of non-government organisations to deliver child protection services. It expects to implement these remaining nine recommendations by the end of 2021.
In addition to the reform, entities have willingly reviewed their practices, policies, and systems to identify opportunities to improve. In particular, the Department of Child Safety has been proactive in looking for better ways to deliver its services to ensure the safety of children. This includes reviewing its investigation and assessment strategy to identify opportunities to streamline its investigation process and engaging a private firm to review the intake system.
Despite the significant reform that has occurred, not all the intended outcomes have been realised. The 10-year reform program proposed by the Carmody Inquiry estimated long-term cost savings to the child protection system through investment in family support services. These savings have not yet been realised.
Between 1 July 2015 and 30 June 2019, the Queensland Government invested over $400 million to implement the reforms. In 2018–19, the Department of Child Safety reported that the number of children coming into the child protection system had not decreased as anticipated by the Carmody Inquiry. As a result, the Queensland Government is funding an additional $401.6 million to continue the reforms to 30 June 2024. Appendix C shows the timelines of reform funding.